

Advancing Health Podcast
AHA Comments on CMS' FY 2027 Proposed Joint Replacement Expanded Model
June 9, 2026
The Honorable Mehmet Oz, M.D.
Administrator
Centers for Medicare & Medicaid Services
7500 Security Boulevard
Baltimore, MD 21244-1850
Submitted Electronically
RE: CMS–1849–P Medicare Program; Hospital Inpatient Prospective Payment Systems for Acute Care Hospitals (IPPS) and the Long-Term Care Hospital Prospective Payment System and Policy Changes and Fiscal Year (FY) 2027 Rates; Requirements for Quality Programs; and Other Policy Changes
Dear Administrator Oz:
On behalf of our nearly 5,000 member hospitals, health systems and other healthcare organizations; our clinician partners — including more than 270,000 affiliated physicians, 2 million nurses and other caregivers — and the 43,000 healthcare leaders who belong to our professional membership groups, the American Hospital Association (AHA) appreciates the opportunity to comment on the Centers for Medicare & Medicaid Services’ (CMS’) proposed Comprehensive Care for Joint Replacement Expanded (CJR-X) Model. We are submitting separate comments on the agency’s proposed changes to the inpatient and long-term care hospital prospective payment systems (PPSs).
Hospitals and health systems are eager to advance value-based care arrangements that improve quality, enhance patient outcomes and make health care more affordable. The AHA and its members support continued innovation in Medicare payment models that align incentives, promote coordinated care and reward prevention and wellness. While we appreciate CMS’ efforts to expand the reach of value-based models, we believe that mandatory participation in the CJR-X Model would present significant challenges, particularly for hospitals that lack the scale or financial capacity to make the necessary investments in care redesign. A phased or voluntary approach would better support success, allowing organizations to build the infrastructure and partnerships needed to achieve shared savings and improved outcomes.
The CJR-X Model, as proposed, includes design elements that would make it difficult for hospitals to be successful under the model. To optimize the effectiveness of CJR-X in terms of how to best transform care delivery through improved care coordination and financial accountability, hospitals must have the necessary tools to succeed and appropriately balance risk versus reward. Specifically, we urge the agency to adopt the following changes to the model in the final rule:
- Make Participation Voluntary. A voluntary pathway to participation would provide a stronger foundation for hospitals to succeed in the model. We urge CMS to give all hospitals the choice to participate in CJR-X. At a minimum, the agency should allow certain categories of hospitals to opt in to the model voluntarily, including those that have participated in bundled payment models and other alternative payment models (APMs), as well as rural, Medicare-dependent, sole community and safety-net hospitals (referred to as “special designation hospitals” herein).
- Create a Glide Path to Risk. CJR-X is the first expanded nationwide mandatory model for hospitals, and as such, a higher bar for introducing downside risk should be set. We recommend that year one of CJR-X be a data-sharing period only, followed by at least two years of no downside risk for all participants as well as upside-only risk for special designation hospitals for the model’s entire duration.
- Eliminate the Discount Factor. A discount factor is not sustainable for a mandatory expanded nationwide model of indefinite duration. This is even more true considering how extensively bundling for joint replacements has already been tested. Therefore, CMS should not finalize any discount factor for CJR-X. If the agency were to adopt a discount factor, it should be set well below 2% and phased out entirely after three years.
- Address the Ratchet Effect. A discount factor combined with annual rebasing of regional target prices means that CJR-X has the potential to be nothing more than a payment cut for hospitals nationwide. We urge CMS to adopt policies to mitigate the ratchet effect of the model that, as proposed, would make continued savings unachievable for hospitals. In addition to no discount factor, the timeframe for rebasing should be extended to, at most, once every ten years.
- Increase the Low-volume Threshold. A low-volume threshold of 31 cases, as proposed, would fail to ensure that hospitals have enough cases to integrate changes in care delivery and determine if they had an impact based on statistical significance. We urge CMS to substantially increase the low-volume threshold to ensure statistical significance and effectively mitigate potential impacts of outliers and volatility in cases.
- Revise the Maximum Stop-loss Limit. The maximum stop-loss limit should be phased in gradually over a period of at least five years. Additionally, it should be no more than 10% for most CJR-X participants and 2.5% for special designation hospitals (to the extent they are subject to downside risk at all).
- Modify the Quality Measures Set. The quality performance aspects of CJR-X should fairly and appropriately reflect relevant care. We have conceptual concerns with some of the proposed measures that we urge CMS to consider and monitor for unintended consequences, as, for most of these measures, it is the first time they are being deployed as part of a pay-for-performance model.
- Waive Applicable Fraud and Abuse Laws. We urge CMS to waive applicable provisions of the Physician Self-Referral Law, the Anti-Kickback Statute and the Beneficiary Inducements Civil Monetary Penalty Law so that organizations can form the financial arrangements necessary to implement CJR-X.
- Extend Medicare Program Waivers to Support Care Delivery. We urge CMS to give providers maximum flexibility to place beneficiaries in the clinical setting that best serves their short- and long-term recovery goals through additional waivers of Medicare program requirements.
The changes we recommend would help facilitate hospitals’ success in providing quality care to Medicare beneficiaries, achieving savings for the Medicare program and pursuing an opportunity for reward that is commensurate with the risk they are assuming. We appreciate your consideration of these issues. Our detailed comments are attached. Please contact me if you have questions or feel free to have a member of your team contact Robyn Tessin, AHA director of payment policy, at rtessin@aha.org.
Sincerely,
/s/
Ashley Thompson
Senior Vice President
Public Policy Analysis and Development
Cc: Abe Sutton
Director, Center for Medicare and Medicaid Innovation
Background
The CJR Model was a mandatory alternative payment model tested by the Center for Medicare and Medicaid Innovation (CMMI) from 2016 through 2024 for certain hospitals in selected Metropolitan Statistical Areas. The model was designed to improve care for Medicare beneficiaries undergoing lower extremity joint replacement (LEJR) performed in the inpatient or outpatient setting. CMS proposes to expand CJR to all eligible hospitals nationwide based on its evaluation results indicating the model successfully reduced spending without reducing quality of care and the Secretary of Health and Human Services’ determination that the model has met the statutory requirements for expansion.
Participation
CJR-X would begin on Oct. 1, 2027. CMS proposes that all acute care hospitals located in the 50 states, the District of Columbia and the U.S. territories and that are paid under both the inpatient and outpatient PPSs would be required to participate, except for hospitals participating in the Transforming Episode Accountability Model (TEAM) and those located in Maryland. The agency notes that hospitals participating in TEAM would be required to participate in CJR-X when TEAM ends or in the event they no longer meet the criteria for inclusion in TEAM.
Mandatory Participation
We are concerned that many hospitals are not in a position to support the investments necessary to transition to a mandatory bundled payment approach for one of the most common surgical procedures in the Medicare patient population. We urge CMS to give all hospitals the choice to participate in CJR-X. We have particular concerns over mandatory participation for certain categories of hospitals, as outlined below, due to, for example, their safety net or other special designation status as well as prior participation in LEJR bundles.
Voluntary Participation Would Support Hospital Success
Hospitals are committed to innovative payment approaches that reward better care, improve patient outcomes and lower the overall cost of care delivery. While we commend CMS’ intention to accelerate the transition to value-based care, mandatory participation in CJR-X would create real barriers, particularly for hospitals that do not have the scale, capital or operational capacity to support significant transformation efforts. A voluntary pathway to participation would provide a stronger foundation for success, giving organizations the flexibility to build needed capabilities and progress toward achieving savings and improved patient outcomes.
Voluntary participation is particularly important because hospitals currently face the competing demands of multiple mandatory CMMI models, especially health systems with multiple locations. As a field, hospitals must contend with not only TEAM, but also the Increasing Organ Transplant Access Model and the Ambulatory Specialty Model that is mandatory for their employed physicians and practitioners. Further, while the Wasteful and Inappropriate Service Reduction Model is voluntary for participating technology companies, hospitals in selected states are forced to adhere to its prior authorization and prepayment medical review requirements.
These concurrent obligations present significant operational and resource challenges, particularly for health systems with multiple hospitals and clinicians participating in different models simultaneously. Each model carries distinct rules, reporting requirements and compliance obligations, increasing administrative burden and introducing the potential for misaligned or conflicting incentives. Moreover, participation across multiple models complicates efforts — both for providers and CMS — to evaluate the effectiveness of specific interventions and determine which approaches are successful.
In addition, although we support CMS adopting successful model design elements at a greater scale across Medicare, we question how much value remains to be gained from LEJR bundled payment models. As discussed below in the Pricing and Payment Methodology section, CJR-X would require participation from hospitals even if they previously participated in CJR and Bundled Payments for Care Improvement Advanced (BPCI-A) and reasonably have little further cost savings to achieve. Specifically, due to the ratchet effect over time, many organizations have squeezed as much cost savings and quality improvement out of LEJR bundles as they can. Thus, they would now simply be taking a payment cut when participating in this model. In addition, our analysis shows that the majority of costs in CJR-X episodes are incurred during the anchor hospitalization or procedure, for which reimbursement is already paid on a bundled basis, leaving few opportunities for savings by participants.
Voluntary participation in CJR-X also would be appropriate given the historic financial pressures that hospitals and health systems continue to face. Indeed, according to the Medicare Payment Advisory Commission (MedPAC) March 2026 report to Congress, inpatient PPS hospitals’ aggregate Medicare margins were a staggering negative 12.1% in FY 2024, and the median margins of even relatively efficient hospitals were negative 1%. Furthermore, MedPAC reported that 18 hospitals closed in the last fiscal year, exceeding the number of hospital openings.1 As such, many hospitals may not be in a position to make the infrastructure investments necessary to be successful in CJR-X, nor absorb potential losses.
Finally, we are concerned that safety-net hospitals and those serving higher proportions of dual-eligible (DE) and low-income subsidy (LIS) beneficiaries in particular may not have the infrastructure and resources necessary to succeed under this model. Our analysis shows that hospitals treating higher complexity and underserved patient populations in LEJR episodes perform categorically worse under CJR-X. Specifically, when we divided hospitals into quintiles based on the difference between their regional target price and spending per episode, we found that hospitals in the highest spending quintile included a disproportionate share of safety-net hospitals and served a disproportionate share of DE or LIS patients (see Table 1).
Table 1. Distribution of Hospital Characteristics for LEJR Episodes by Quintile: Safety-net, DE and LIS
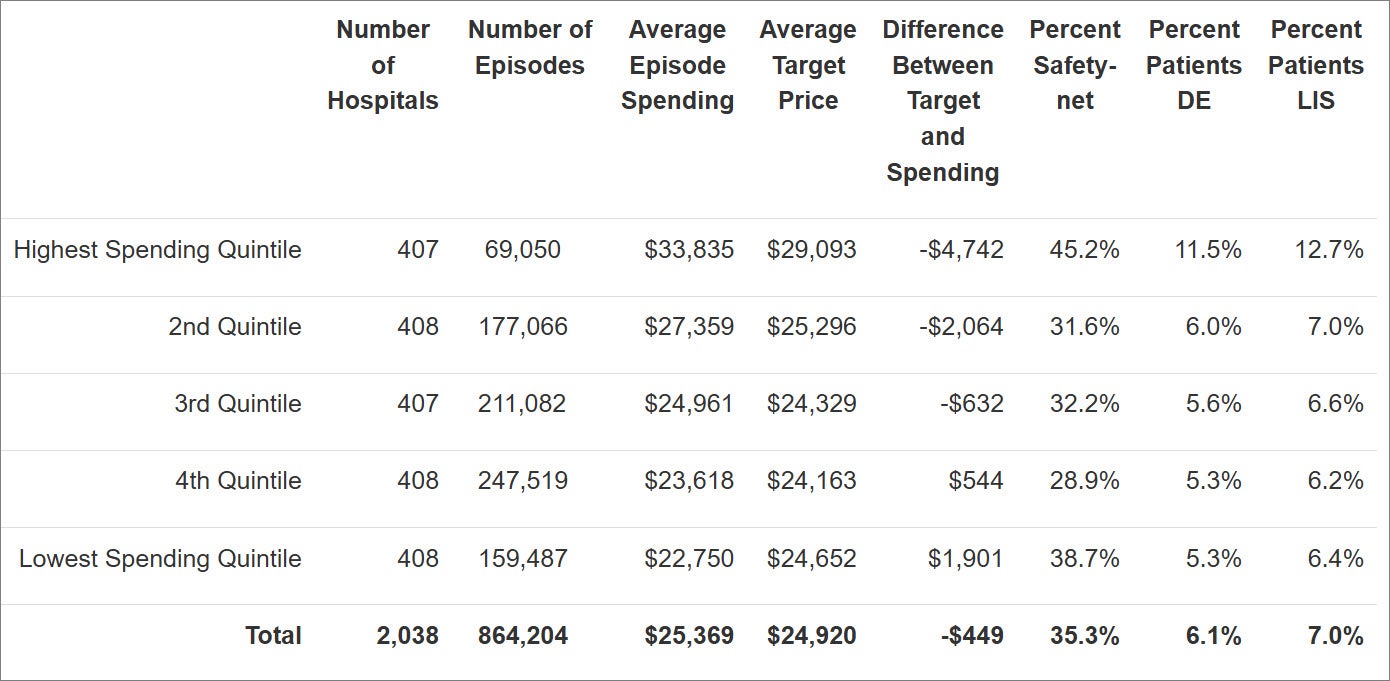
Source: AHA analysis of FY 2023-2025 Medicare claims data.
As such, we are extremely concerned that mandatory participation could contribute to a downward financial spiral for these organizations, which would have even fewer funds to invest in APMs, let alone targeted interventions to benefit their patients and communities. This could in turn lead to even larger losses under the model, eventually resulting in decreased access to care and widening disparities for underserved populations.
Participant Exclusions
Exclusion of TEAM and Maryland Hospitals
We support CMS’ proposal to exclude hospitals participating in TEAM and those located in Maryland from CJR-X. However, we disagree that TEAM hospitals should be required to participate in CJR-X when TEAM ends or in the event they no longer meet the criteria for inclusion in TEAM. These hospitals will have already implemented care redesign for LEJR episodes and achieved efficiencies under an even shorter 30-day episode timeframe in TEAM. Many TEAM hospitals may be unable to achieve further savings or quality of care improvements with LEJR episodes, and thus they should be given the choice to opt in to CJR-X.
Voluntary Opt-in for CJR and BPCI-A Participants
CJR-X would mandate participation from hospitals that participated in CJR and BPCI-A, even though they have likely exhausted opportunities to reduce spending associated with LEJR procedures. As mentioned above regarding TEAM hospitals, many of these organizations have already captured achievable efficiencies for LEJR episodes. As a result, mandating their participation in CJR-X would set them up for failure and would effectively translate into a permanent payment cut on these procedures. Thus, we urge CMS to allow CJR and BPCI-A participant hospitals to choose whether to participate in CJR-X.
Voluntary Opt-in for Hospitals Participating in Other APMs
Hospitals participating in other APMs also should be allowed to voluntarily opt in to CJR-X. The staffing and resources required for one hospital to participate in multiple APMs are significant, particularly if they are being implemented at the same time. There also is the potential for organizations to be penalized in multiple models for the same cases and measures because, aside from TEAM, model interactions are not accounted for in the CJR-X proposal. Some examples are noted below.
Achieving Healthcare Efficiency through Accountable Design (AHEAD) Model Hospital Participants
Hospitals that participate in AHEAD already will be undergoing significant organizational change and redesign of care pathways for all of their clinical areas, including LEJR. Measuring these episodes twice would be inappropriate and untenable. In addition, the AHEAD and CJR-X performance periods would overlap, and it would be difficult to discern which model interventions would be responsible for changes in outcomes.
IOTA Model Hospital Participants
The mandatory IOTA Model began on July 1, 2025, for kidney transplant hospitals in selected areas. Again, implementation of complex payment models requires significant time, resources and staffing on the part of hospital participants. With a six-year performance period, IOTA hospitals could be implementing multiple models at the same time (for example, IOTA, TEAM and AHEAD, not to mention any other voluntary models).
Accountable Care Organization (ACO) Hospital Participants
ACO models are intended to hold organizations accountable for aggregate healthcare expenditures and population health outcomes for an attributed population. Requiring ACO participants to also participate in CJR-X could result in duplication of effort, as ACOs already support episode management post-discharge and redirection of resources.
Voluntary Opt-in for Special Designation Hospitals
As previously mentioned, rural, Medicare-dependent, sole community and safety-net hospitals have less infrastructure and resources available to implement a mandatory bundled payment model. They also would be disproportionately at risk for losses under CJR-X because of the more medically complex patient populations they serve. As such, these organizations should have the flexibility to opt in to CJR-X.
View the full letter below.
__________
1 https://www.medpac.gov/wp-content/uploads/2026/03/Mar26_Ch3_MedPAC_Report_To_Congress_SEC.pdf
Key Resources
Related Resources
Webinar Recordings