

Advisories
AHA Comments on CMS' FY 2027 Inpatient Proposed Payment Rule
June 9, 2026
The Honorable Mehmet Oz, M.D.
Administrator
Centers for Medicare & Medicaid Services
7500 Security Boulevard
Baltimore, MD 21244-1850
RE: CMS-1849-P, Medicare Program; Hospital Inpatient Prospective Payment Systems for Acute Care Hospitals (IPPS) and the Long-Term Care Hospital Prospective Payment System and Policy Changes and Fiscal Year (FY) 2027 Rates; Requirements for Quality Programs; and Other Policy Changes, (Vol. 91, No. 71), April 14, 2026.
Dear Administrator Oz:
On behalf of our nearly 5,000 member hospitals, health systems and other healthcare organizations, our clinician partners — including more than 270,000 affiliated physicians, 2 million nurses and other caregivers — and the 43,000 healthcare leaders who belong to our professional membership groups, the American Hospital Association (AHA) appreciates the opportunity to comment on the Centers for Medicare & Medicaid Services (CMS) hospital inpatient prospective payment system (PPS) proposed rule for fiscal year (FY) 2027. We are submitting separate comments on the agency’s proposed changes to the long-term care hospital (LTCH) PPS and the Comprehensive Care for Joint Replacement Expanded Model.
America’s hospitals and health systems are the backbone of the U.S. healthcare system, providing 24/7 care to patients and communities. Hospital care today is more advanced, more effective and more resource-intensive than ever, reflecting major gains in medical innovation, as well as the highly skilled workforce, technology and infrastructure required to deliver it. Patients are living longer, recovering faster and receiving treatments that would have been unimaginable just a generation ago. As communities across the country face demand for health services, it is essential that Medicare payment policies support the sustainability and availability of these providers.
To that end, we support several of the inpatient PPS proposed rule provisions, including the proposed updates to define “new” residency programs under the graduate medical education policies. We also support the removal of measures from the quality reporting program that are no longer providing useful information to improve patient outcomes and are optimistic about CMS' work to develop a more robust measure of sepsis mortality.
At the same time, we continue to have strong concerns about the proposed payment update. The proposed net payment update of 2.4% is not adequate given the unrelenting financial headwinds hospitals and health systems face. We are particularly concerned with the inappropriately large proposed productivity cut. Therefore, we ask CMS to work with Congress to reduce the magnitude of the productivity adjustment.
We also have serious concerns over the agency’s estimates to calculate disproportionate share hospital (DSH) and uncompensated care payments. These proposed payments are half a billion less than what hospitals received last year. We expect the uninsured rate to be higher than what CMS currently proposes. However, the lack of transparency on these estimates severely limits our ability to sufficiently comment on the agency’s methods and calculations. We urge CMS to publish a detailed methodology so that stakeholders can sufficiently comment on the issue.
Finally, we also are concerned that CMS has not provided adequate analysis to demonstrate that the inclusion of Medicare Advantage enrollees in quality measure denominators will not result in unfair comparisons across providers based on the markets in which they serve rather than on the quality of care they provide. This is particularly troubling in the Hospital Readmissions Reduction Program, where performance influences payment adjustments.
We appreciate your consideration of these issues. Our detailed comments are attached. Please contact me if you have questions or feel free to have a member of your team contact Shannon Wu, AHA director for payment policy, at (202) 626-2963 or swu@aha.org.
Sincerely,
/s/
Ashley Thompson
Senior Vice President
Public Policy Analysis and Development
INPATIENT PPS PAYMENT UPDATE
The AHA remains concerned that CMS’ proposed annual market basket update of 3.2% is not keeping pace with real-world cost growth. In recent years, CMS’ market basket forecasts have consistently come in below broader inflation, let alone medical inflation, which has exceeded growth in the overall economy. Layered on top of that, the productivity adjustment, proposed to be 0.8 percentage points for FY 2027, further erodes the update, leaving Medicare payments increasingly out of sync with the cost of care. We urge CMS to revisit both its market basket forecasts and the magnitude of the productivity adjustment, and to consider the combined effect on provider reimbursements. As such, we ask CMS to work with Congress to reduce the magnitude of the productivity adjustment.
Rising Costs of Care Continue to Strain Healthcare Providers
Hospitals and health systems continue to face serious inflationary pressures. As detailed in our comments on the FY 2026 inpatient PPS proposed rule, unprecedented levels of inflation have raised labor, drug, supply and other costs. A recent AHA report found that total hospital expenses increased by 7.5% in 2025 alone.1 Much of this increase reflects labor costs, which CMS notes account for more than half of the inpatient market basket. Indeed, an AHA analysis found that workforce costs rose by 5.6% in 2025.2 Further, advertised salaries for registered nurses have averaged 5.5% growth over the last two years — more than double the rate of inflation.3 Finally, the AHA has expressed concern that recent actions, such as changes to federal student loan limits that exclude nurses and other clinicians from enhanced borrowing limits, will exacerbate workforce shortages, which contribute to higher costs for labor.
Cost pressures, however, extend well beyond labor. Like other providers, hospitals are increasingly caring for sicker and more complex patients, requiring additional and more costly drugs and supplies, and these costs also continue to climb. An AHA analysis showed that in 2025, supply costs rose 9.9%, while drug costs rose a staggering 13.6%.4 In fact, 19% of hospital cost growth is driven by the services to care for sicker and more complex patients, as hospitals devote more staff time, monitoring and specialized treatment to each case. Another 45% of hospital cost growth can be attributed to higher input costs per patient, such as rising wages and benefits for clinical and other staff, and higher prices for drugs, supplies and equipment. These cost challenges strain hospitals and health systems, which must be prepared to provide treatment for a wide range of conditions and comorbidities.
Providers also are absorbing escalating administrative costs that are not reflected in payment updates. In addition to direct costs of care, hospitals have also faced rising administrative costs. For example, the vast majority of Medicare Advantage (MA) plans require prior authorizations. As such, hospitals and health systems spend substantial amounts of time and resources navigating the prior authorization process. In 2025, hospitals spent nearly $18 billion on overturning claims denials alone.5 All told, using data from the most recent annual survey, the AHA estimates that hospitals spent a staggering $43 billion in 2025 trying to collect payments insurers owe for care already delivered. In 2024, the average hospital employed about 64 administrative and billing staff dedicated to these functions — roughly 6.5% of total hospital employment — according to AHA analysis of annual survey data. Notably, many of these denials were ultimately overturned as noted above. In fact, a study by the Health and Human Services Office of Inspector General found that 75% of care denials were subsequently overturned.6 Making matters worse, MA plans paid hospitals less than 90% of Medicare rates despite costing taxpayers substantially more than traditional Medicare in 2023.7,8 Since plans do not reimburse these administrative expenses, providers must absorb them while caring for a growing share of MA patients.
Viewed collectively, these cost increases for staffing, drugs and other essential supplies and services are placing significant strain across the healthcare continuum. They also are forcing providers to redirect resources that otherwise could be used to support patient care, adopt new technologies and make other efficiency-enhancing investments. That reality makes CMS’ insufficient market basket updates, which fall well below the levels of growth observed in labor, drugs, supplies and other costs, even more troubling. As discussed further below, these same pressures also amplify the negative impact of the productivity adjustment on providers’ ability to fund the very investments that can drive operational efficiencies.
Severe Medicare Underpayments Cannot Be Sustained
During this period of significant cost growth, the market basket forecasts for inpatient hospitals consistently failed to accurately predict actual market basket growth. We have detailed these under-forecasts of the market basket and potential drivers of that under-forecast in our past comments. While forecasts will never be perfect, in the past, they have been more balanced. AHA continues to stand ready to work with CMS to examine the market basket compensation indices and proxies to improve the accuracy of these measures.
Indeed, these trends have continued and exacerbated Medicare’s underpayments to the hospital field. The Medicare Payment Advisory Commission projects that 2026 Medicare margins will be negative 10%, resulting in more than 20 straight years of Medicare paying below costs.9 The AHA’s own analysis showed that Medicare underpayments reached $100 billion in 2024.10 This is unsustainable. Therefore, we urge CMS to focus on appropriately accounting for recent and future trends in inflationary pressures and cost increases in the hospital payment update, which is essential to ensure that Medicare payments for acute care services more accurately reflect the cost of providing hospital care.
The Productivity Adjustment Exacerbates Insufficient Market Basket Updates
Under the Affordable Care Act (ACA), the inpatient PPS payment update is reduced each year by a productivity factor equal to the 10-year moving average of changes in the annual economy-wide, private nonfarm business total factor productivity (TFP). The private nonfarm business TFP is intended to reflect gains from new technologies, economies of scale, business acumen, managerial skill and changes in production. As such, it effectively assumes that the hospital field can achieve productivity gains comparable to those realized by private nonfarm businesses. However, as discussed in more detail below and in a report shared last year, the healthcare field cannot mirror these gains. As a result, it is not an appropriate or reliable proxy for healthcare productivity. Therefore, we ask CMS to work with Congress to reduce the magnitude of the productivity adjustment.
A core problem is that the productivity construct embedded in the private nonfarm business TFP is a poor fit for measuring healthcare productivity. TFP outputs are measured based on the total quantity and prices of goods and services produced in private nonfarm businesses. In industries that sell tangible products, outputs can often be measured in relatively straightforward and standardized ways. Healthcare outputs, however, do not operate in the same manner. For example, healthcare “quantity,” such as volume of visits or procedures, is not necessarily an appropriate proxy for output; it may instead reflect the underlying disease burden in a community. More provider volume — i.e., more quantity — does not equate to higher productivity in the way it can for private nonfarm businesses.
Further, providers often cannot adjust prices per unit of service in response to changes in demand or quality in the way private nonfarm businesses can. Much of hospitals' and health systems' reimbursement is paid through fixed payment systems, such as the inpatient PPS, which limits providers’ ability to alter prices. Similar constraints apply in the commercial market: providers do not unilaterally set their rates, and prices for commercially insured patients are established through negotiations that frequently lock in rates for multiple years. Accordingly, applying a TFP output framework based on quantity and prices — as experienced in the private sector — to healthcare providers is problematic because that output function does not translate to the healthcare field.
In addition, the hospital field also differs from many private nonfarm industries because healthcare services are inherently labor-intensive. As discussed further in the report referenced above, economic literature has long recognized that sustained productivity gains are difficult to achieve in labor-intensive service industries because labor cannot be scaled or automated in the same way as in other sectors. In this respect, healthcare providers are more comparable to fields such as education and social assistance, which tend to experience lower total factor productivity rates. For example, Bureau of Labor Statistics data show rates ranging from -0.4 for educational services to -0.1 for social assistance, compared with 1.9 to 4.9 for industries such as mining, oil and gas, information, and professional services.
Finally, we continue to find it especially troubling that the productivity adjustment appears to be applied only when it reduces Medicare payments. For example, in FY 2021, the 10-year moving average growth of the productivity factor forecast was ‑0.1%. CMS acknowledged that subtracting a negative growth factor from the market basket would have increased it by 0.1 percentage point. However, the agency set the productivity factor at 0, stating that it is required to reduce — not increase — the market basket by changes in economy-wide productivity.11 Put simply, the agency uses the productivity factor only when it lowers Medicare spending.
The cumulative, compounding effect of these annual reductions — coupled with the asymmetric treatment of periods of declining economy-wide productivity — has widened the gap between payments and the cost of providing services, leaving providers increasingly underfunded, as discussed above. In light of the above, the AHA continues to have serious concerns about the proposed productivity cut, particularly given the extraordinary pressures under which healthcare providers continue to operate.
INPATIENT PPS OUTLIER THRESHOLD
The AHA is concerned about the proposed increase in the high-cost outlier threshold. It represents a 28% increase from the FY 2026 threshold and, as such, would significantly decrease the number of cases that qualify for an outlier payment. We are further concerned that it is coming after CMS has already increased the threshold substantially in the past years. Indeed, the chart below details the increase in the outlier threshold over the past 19 years — a staggering 158% increase from FY 2009 through FY 2027 (as proposed).
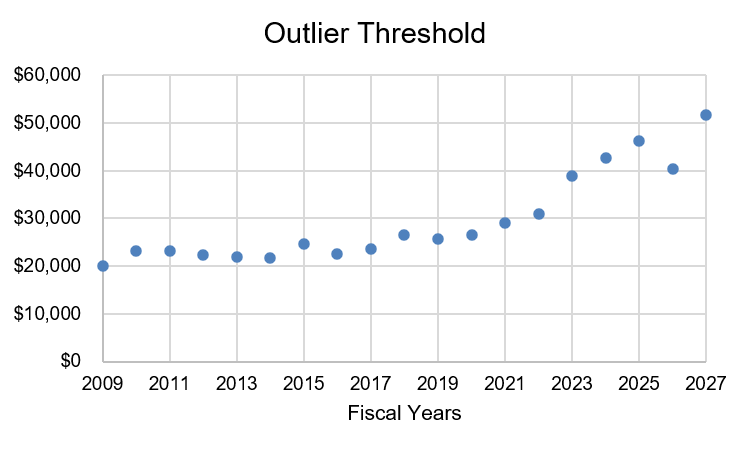
This large increase seems to be a result of the agency using the change in average charges from FY 2024 to FY 2025 to determine a charge inflation factor (CIF) and then using this factor to estimate the charge inflation for FY 2027. Indeed, the proposed charge inflation for FY 2027 is noticeably higher than FY 2026 — 15.154% compared to 11.313%. We ask that the agency examine its charge inflation methodology and the appropriateness of using two-year delayed data to estimate current year charge inflation. We urge the agency to make additional, temporary changes to help mitigate the substantial increases occurring in the outlier threshold.
MEDICARE DISPROPORTIONATE SHARE HOSPITAL PAYMENT
Under the DSH program, hospitals receive 25% of the Medicare DSH funds they would have received under the former statutory formula (described as “empirically justified” DSH payments). The remaining 75% flows into a separate funding pool for DSH hospitals. This pool is reduced as the percentage of uninsured declines and is distributed based on the proportion of total uncompensated care each Medicare DSH hospital provides.
Transparency Related to DSH Calculations
The AHA remains concerned about the lack of transparency on how CMS and the Office of the Actuary (OACT) calculate DSH payments. As we have previously commented, we urge the agency to disclose the OACT information outlined below in advance of publication of the final rule and permit further comment on it. Moreover, we urge the agency to disclose such information in its inpatient PPS proposed rule each year in the future.
Factor 1
Factor 1 is the estimate of what total DSH payments would have been under the former statutory formula. In estimating Factor 1, CMS used a variety of data inputs, which it included in a table detailing the factors applied for FYs 2024 through 2027.12 In this table, the agency includes a “Discharges” column that shows changes in the number of Medicare fee-for-service (FFS) inpatient hospital discharges, with FY 2026 and FY 2027 figures based on historical experience and assumptions related to how many beneficiaries will be enrolled in MA plans. However, the agency provides no other details on how this historical experience or assumptions on MA enrollment are obtained to arrive at these estimates.
Additionally, the table also includes a “Case-mix” column that shows the estimated change in case-mix for inpatient PPS hospitals. CMS states that FY 2027 case-mix is based on assumptions from the 2012 “Review of Assumptions and Methods of the Medicare Trustees’ Financial Projections” report by the 2010-2011 Medicare Technical Review Panel. This report utilizes data from the 1980s up until 2010.13 The report itself states that “growth in the average complexity (or intensity) of healthcare services is an important element of Medicare expenditures … and that case-mix increases usually occur as a result of the development and diffusion of new medical technology.” The report, at that time, had concluded “that a short-range (emphasis added) case-mix assumption […] would be more representative than the current assumption.” Yet, CMS still chooses to utilize assumptions from this report that, at best, describe case-mix from 16 years ago. In other words, it takes the very action that the report effectively cautions against. As such, we question the continued use of assumptions from a report that used data that is, at best, 16 years out of date.
Finally, the table includes an “Other” column that the agency says “reflects the change in other factors that contribute to the Medicare DSH estimates,” including the difference between total inpatient hospital discharges and inpatient PPS discharges, and various adjustments to the payment rates that have been included over the years but are not reflected in the other columns. In past years, CMS has described in more detail adjustments that contribute to these estimates. For example, in the FY 2026 proposed rule, CMS stated that this column “includes a factor for the estimated changes in Medicaid enrollment through FY 2023.”14 For this year’s proposed rule, however, the agency has removed its prior-year descriptions and offers no details on the factors that contribute to this column, which makes it virtually impossible for stakeholders to comment on the estimated impacts of Medicaid changes during such a critical time.
Given the administration’s interest in transparency, we urge the agency to detail its calculations. Specifically, we respectfully request that it publish a detailed methodology of its calculations that specifies how all the components contribute, as well as their estimates from year to year, so that stakeholders can sufficiently comment on the issue.
Additionally, the AHA urges CMS to publish detailed calculations of the discharge estimates in the inpatient PPS proposed rule each year going forward, so there is sufficient information to evaluate the impact on FFS inpatient hospital payments and provide feedback to the agency on how growth in MA is affecting the development of FFS rates over time. The growth of MA has led to frustrations around, for example, prior authorization requirements placed by plans, which often negatively impact patients and providers alike.15 As such, there are questions about the sustainability of MA growth and its impact on inpatient hospital payments, and in particular, on those hospitals that serve a disproportionate share of lower-income beneficiaries. The AHA welcomes the opportunity to work with CMS in examining the impacts of MA enrollment on FFS inpatient hospital payments.
Factor 2
CMS establishes Factor 2 in the calculation of uncompensated care DSH payments as one minus the percent change in the percent of uninsured individuals, determined by comparing the percent of the individuals who were uninsured in 2013 and the percent of individuals who were uninsured in the most recent period for which data is available. In the FY 2026 final rule, CMS used an uninsured rate of 8.7% for FY 2026. In this rule, CMS proposes to use an uninsured rate of 9.1% for FY 2027. Given potential and realized Medicaid and enhanced ACA premium tax credit policy changes, we believe we will see a much larger increase in the number of uninsured than the agency proposes.
To determine uninsured rates, OACT uses projections from the latest National Health Expenditure Accounts (NHEA) historical data, which account for expected changes in enrollment across several categories of insurance coverage, including Medicaid. OACT projects enrollment and spending trends for the coming 10-year period; the most recent projections are for 2024 through 2033 and use NHEA historical data through 2023. OACT utilizes NHEA projections, which estimate that in 2026, the uninsured growth rate will be 15.2%, but that in 2027 the rate will be 1.0%. Furthermore, NHEA projects that the Medicaid enrollment growth rate will be 2.1% for 2026 and 2027.16 We question these estimates.
For example, recent estimates suggest that plan sign-ups for the ACA Marketplace fell by over a million people during the 2026 open enrollment period, the sharpest single-year drop since the ACA Marketplace launched.17 Effectuated enrollment — the number of people who pay premiums and maintain effective coverage — is expected to fall substantially. Accounting for unpaid premiums, mid-year attrition and other factors, it is estimated that the average effectuated enrollment could decline by between 17% to 26% in 2026. Furthermore, a recent survey conducted in spring 2026 showed that 9% of 2025 Marketplace enrollees had become uninsured, 4% of returnees had not paid their first month’s premiums, and 17% of returning enrollees were not confident they could pay premiums for the entire year. As the fallout of the expiration of the enhanced premium tax credits continues to play out for the remainder of 2026 and into 2027, it is clear that the uninsured rate will continue to rise substantially.
Similarly, the Congressional Budget Office’s (CBO) estimate of the One Big Beautiful Bill Act projects that almost eight million people will become uninsured.18 Specifically, one Medicaid provision alone — whereby on Dec. 31, 2026, states must start re-determining eligibility expansion enrollees every six months — would result in 11% of the expansion enrollees procedurally disenrolled.19 Also under these estimates, average monthly Medicaid expansion enrollment would be reduced by 17%. CBO also estimates that the uninsured will increase by 1.3 million in 2026 and 5.2 million in 2027.20 Given these estimates, we question the National Health Expenditure Data’s (NHEA) conclusion that Medicaid enrollment will continue to grow in 2026 and 2027.
In such a climate of continued turbulent coverage losses, we urge CMS to carefully consider its reliance on current data sources and methodologies to estimate the uninsured rate. Data and projections that worked when coverage levels were more stable may no longer be adequate.
Finally, CMS also does not publish its Factor 2 methodology, which severely limits the AHA’s ability to sufficiently comment on this issue. Specifically, the agency has not published the details of its methodology and how it incorporates NHEA projections, despite stakeholders, including the AHA, consistently voicing their concerns. As such, we urge CMS to not only publish a detailed methodology on the Factor 2 calculation and how it uses and incorporates NHEA projections, but also to use real-world data from key stakeholders and researchers to arrive at a more appropriate uninsured estimate.
Use of Worksheet S-10 Data
CMS proposes to use three years of audited data to determine uncompensated care payments in FY 2027. Specifically, the agency proposes to use the three-year average of uncompensated care from the three most recent FYs for which audited data are available.
The AHA has a longstanding position supporting the use of audited S-10 data to promote accuracy and consistency. We continue to believe that audited data and, by extension, ongoing refinements to the audit process, result in data that are most appropriate for use in Medicare DSH payments. In addition, three-year averages help to reduce year-to-year fluctuations, providing more predictability and stability for hospitals. We, therefore, support CMS’ proposal to use the three most recent FYs of S-10 data to determine each Medicare DSH hospital’s share of uncompensated care in FY 2027.
We also support the following DSH proposals:
- Newly Merged Hospitals. CMS proposes to continue its policy to treat hospitals that merge after the development of the final rule as new hospitals. Specifically, the newly merged hospital’s (i.e., the surviving hospital’s) current cost report would be used to determine the hospital’s DSH payment. CMS also proposes to continue its policy that interim uncompensated care payments for the newly merged hospital would be based only on the data for the surviving hospital’s CMS Certification Number available at the time of the development of the final rule. CMS would then determine the final DSH payment for the newly merged hospital during the FY 2026 cost report settlement.
- New Hospitals. CMS proposes to continue its policy for new hospitals. Specifically, for newly established hospitals, the hospital’s Medicare Administrative Contractor (MAC) would make a final determination concerning whether the hospital is eligible to receive Medicare DSH payments at the cost report settlement.
Section 1115 Waiver Days
In 2023, the Biden administration implemented a policy that penalizes non-expansion states, rewriting long-standing policy without congressional authorization and putting safety-net hospitals at risk in the process. Specifically, CMS will not allow hospitals to include CMS-approved Section 1115 waiver days associated with uncompensated care pools in the Medicare DSH calculation.
AHA has consistently emphasized that this policy is inconsistent with the plain language of the Medicare statute and decades of policy and practice.21,22,23 The statute directs that the Medicaid fraction capture patient days for individuals “eligible for medical assistance under a State plan approved under title XIX,” and longstanding policy recognized that individuals served through Section 1115 demonstrations, including uncompensated care pools, fall within this framework. CMS’ reinterpretation improperly narrows the statute by imposing additional criteria that are not supported by the law.
In addition, AHA has underscored that CMS’ repeated attempts to exclude these days, described in agency rulemaking as efforts to limit the counting of uncompensated care pool days, would materially reduce the number of Medicaid days included in the DPP calculation.
This policy, in turn, will have significant adverse consequences for hospitals that serve a disproportionate share of low-income and vulnerable patients. By reducing DSH payments, the policy would undermine a critical source of financial support hospitals depend on to furnish essential services in underserved communities. AHA has expressed concern that these reductions could jeopardize access to care for low-income populations and exacerbate existing health disparities, particularly in states that have not expanded Medicaid and rely heavily on Section 1115 demonstrations to finance care for uninsured and underinsured individuals.
Finally, AHA has noted that the policy would introduce unnecessary complexity and administrative burden by requiring hospitals to distinguish among categories of Section 1115 enrollees and verify detailed coverage criteria, while disregarding the practical realities of how states structure Medicaid coverage through demonstrations. These changes would disrupt settled expectations, create operational challenges and inject further instability into the DSH payment methodology.
For these reasons, AHA is asking CMS to consider restoring the historical treatment of inpatient days associated with CMS-approved Section 1115 demonstrations, including uncompensated care pool days, as days for patients “regarded as eligible for medical assistance under a State plan approved under title XIX for purposes of the Medicaid fraction of the Medicare DSH calculation.” And in making this change, we ask CMS to consider allowing hospitals to include these patient days in the Medicaid fraction numerator.
GRADUATE MEDICAL EDUCATION PAYMENTS
Medicare direct GME and indirect medical education (IME) funding are critical to educating the physician workforce and sustaining access to care. Yet, currently insufficient funding levels and limits on the number of residents for whom each teaching hospital is eligible to receive GME reimbursement are major barriers to reducing the nation’s significant physician shortage. CMS proposes several modifications that would affect Medicare GME payments to teaching hospitals.
CMS establishes the rules for applying direct GME and IME caps for new medical residency training programs — those established on or after Jan. 1, 1995. The agency previously defined a “new” residency program and adopted criteria to determine whether a residency program qualifies as “new” for purposes of determining whether a hospital can receive additional direct GME and/or IME slots for that program. Specifically, to be considered a “new” program, a previously non-teaching hospital would have to ensure that the program meets three primary criteria: 1) the residents are new; 2) the program director is new; and 3) the teaching staff are new.
We appreciate that CMS has carefully considered stakeholder comments on its initial set of proposals regarding the newness of a residency program and a related request for information from the field. Specifically, we thank CMS for proposing that it will no longer consider the previous employment of the faculty or program director in determining whether the program director is new for cap building purposes. As we stated in our FY 2025 comment letter, we agree that it is important to have experienced faculty and program directors to stand up new residency programs, where they have the expertise and knowledge of accreditation requirements and how to properly train the next generation of physicians. To combat the current physician workforce shortage and ensure that the field continues to train high-quality physicians, experience is a necessary factor.
After considering stakeholder comments, CMS is proposing that for programs starting on or after Oct. 1, 2026, at least 90% of the individual resident trainees (not full-time equivalents) must not have previous training in the same specialty as the new program. The agency also proposes several exceptions to this rule. Specifically, we had previously expressed our concern that programs may have every intent to meet the threshold of 90% individual trainees being new, but through the binding residency matching program, find themselves unable to meet the threshold. Therefore, we thank CMS for proposing to exclude trainees with previous experience training in another program in the same specialty who enter the new program as first-year residents, recognizing that hospitals should not be penalized for results of the binding matching program and fulfilling the 90% requirement. CMS would also create an exception to the 90% requirement for small residency programs, defined as one accredited for 16 or fewer positions, regardless of whether the program is located in an urban or rural area. We support these proposals.
NURSING ALLIED HEALTH EDUCATION PAYMENTS
Medicare makes payment for its share of a hospital’s reasonable cost for approved nursing and allied health education (NAHE) programs operated by the hospital. These payments play a critical part in training the next generation of health providers.
In last year’s rule, CMS issued a proposal to address a court ruling related to the net costs of NAHE that hospitals are allowed to claim for pass-through payment. The AHA urged CMS to reconsider its proposal. We stated at the time that the proposal could result in circumstances where revenue from or on behalf of students reduces direct NAHE costs to zero, and there would be no indirect costs to allocate. As such, providers could no longer receive NAHE payments, without which they may be forced to close such programs. We appreciate that CMS considered stakeholder comments and modified its proposal in this year’s rule to ensure that the deduction of revenue does not inappropriately reduce the allocation of indirect costs to the NAHE cost center.
However, the AHA remains concerned that portions of the proposed discussion regarding related organizations and indirect costs may not fully reflect the realities of how many NAHE programs operate. Many NAHE programs depend on the centralized administrative resources operated by their hospital to improve efficiency, reduce duplication and better coordinate NAHE programs across all affiliated hospitals. These centralized functions include payroll processing, accounting systems, human resources support, benefits administration and other operational infrastructure. They do not alter the fact that the provider hospitals themselves continue to directly operate and control their NAHE programs, including direct control over curriculum, administration, faculty, and classroom and clinical instruction. We urge CMS to consider that a NAHE program’s use of centralized or shared administrative infrastructure does not, by itself, invalidate hospital-operated status or otherwise preclude allowable NAHE pass-through reimbursement as long as the hospital continues to satisfy the substantive operational control requirements established under the regulation.
AREA WAGE INDEX
Permanent Cap on Wage Index Decreases
In the FY 2024 rule, CMS finalized a policy to apply a 5% cap on all wage index decreases, regardless of the reason, in a budget-neutral manner. For FY 2027, CMS estimates that the cap on reductions will require a budget neutrality adjustment of -0.80%. The AHA appreciates CMS’ recognition that significant year-to-year changes in the wage index can occur due to external factors beyond a hospital’s control. While we support this policy that would increase the predictability of inpatient PPS payments, we continue to urge CMS to apply this policy in a non-budget-neutral manner.
Low-wage Hospital Policy
Beginning in FY 2020, CMS finalized a policy to increase wage index values for low-wage hospitals. This was done in a budget-neutral manner through an adjustment applied to the standardized amounts for all hospitals. Specifically, the agency increased the wage index for hospitals with a wage index value below the 25th percentile by half the difference between its otherwise applicable wage index value and the 25th percentile wage index value across all hospitals for that year. While this policy was originally scheduled to expire after FY 2023, CMS indicated it had been unable to disentangle the effects of the COVID-19 pandemic and the low-wage index policy to determine whether the policy had successfully resulted in hospitals raising wages to get a higher wage index. Therefore, in the FY 2025 proposed rule, the agency proposed to extend the policy and related budget neutrality adjustment for at least three more years.
However, in the FY 2025 final rule, CMS noted that the policy had become the subject of litigation. Specifically, on July 23, 2024, the Court of Appeals for the D.C. Circuit held that the secretary lacked authority to adopt the policy and that it, and its related budget neutrality adjustments, must be vacated. As a result of this court decision, the agency discontinued the low-wage index policy and its related budget neutrality factor for FY 2025. It also implemented a non-budget-neutral transition policy for hospitals impacted by the discontinuation, which capped wage index decreases at 5%.
In the FY 2026 rule, CMS finalized that it would discontinue the low-wage policy for FY 2026 and beyond. Additionally, the agency implemented a budget-neutral policy to help hospitals significantly impacted by the policy removal, capping decreases at 5%. CMS is proposing the same transitional policy done in a budget-neutral way for FY 2027. However, we believe that CMS is not bound by statute to make its proposal budget-neutral. We appreciate that the agency’s FY 2025 transition policy was implemented in a non-budget-neutral manner, and we maintain that the FY 2027 transition policy should also be implemented in a non-budget-neutral manner. Indeed, reducing the standardized amount for all PPS hospitals intensifies historical Medicare underpayment. As such, the AHA urges CMS to implement the FY 2027 low-wage hospital transition policy in a non-budget-neutral manner.
Imputed Rural Floor Calculation
As required by law, CMS proposes to continue the minimum area wage index for hospitals in all-urban states, known as an “imputed rural floor,” for FY 2027. This policy applies to states that have no rural hospitals or no rural areas to set a rural floor wage index for those states. Also, as required by law, CMS proposes to apply this policy in a non-budget-neutral manner. We support this proposal.
RURAL HOSPITAL PROVISIONS
Low-volume Adjustment and Medicare-dependent Hospital Program
The Consolidated Appropriations Act, 2026, extended the low-volume hospital qualifying criteria and payment adjustment (LVA) and the Medicare-dependent Hospital (MDH) Program under the inpatient PPS through Dec. 31, 2026. However, as it currently stands, beginning on Jan. 1, 2027, the LVA would revert to statutory requirements that were in effect prior to FY 2011. Similarly, beginning Jan. 1, 2027, the MDH program would expire. The AHA supports congressional action to make permanent the enhanced LVA so that hospitals can continue to qualify for and be paid under the current enhanced method. We also support congressional action to make permanent the MDH program, with an additional base year available to calculate MDH payments, which would provide more flexibility for these hospitals to provide the best care possible for their patients and communities.
Additionally, we also urge CMS to expeditiously process claims and provide instructions to MACs during program extensions, especially in instances when extensions are made retroactively. Although FFS Medicare makes retrospective payments for program extensions that occur retrospectively, many MA plans do not. That is, until CMS issues instructions to the MACs and updates its databases identifying MDH and LVA hospitals, these hospitals do not receive enhanced Medicare reimbursements from MA plans. These rural hospitals, which are already in vulnerable financial states, are owed tens of millions of Medicare payments as a result of cumbersome administrative processes. Seamless transition of programmatic support is a crucial lifeline for rural providers.
Hospitals Applying for Rural Referral Center Status
One way in which a hospital can qualify for rural referral status is based on a combination of discharge volume and case-mix criteria, in comparison to other providers in the hospital’s region. CMS proposes to use FY 2025 data to calculate case-mix criteria and FY 2024 cost report data to calculate discharge volume. We support the use of this data.
PROPOSED CHANGES TO SPECIFIC MS-DRG CLASSIFICATIONS
Overall, the AHA supports CMS’ proposed changes within the Medicare Severity Diagnosis-Related Group (MS-DRG) Classifications section. We agree with most proposals based on the data analysis presented in this proposed rule. However, we request that CMS consider the exceptions detailed below.
First, the AHA thanks CMS for continuing to provide test versions of files and software applications needed to assess proposed MS-DRG classification changes. Specifically, we thank CMS for providing the draft MS-DRG test GROUPER and Medicare Code Editor (MCE) ICD-10 software Version 44 (V44).
We also value CMS making available the supplemental mapping files in Tables 6P.1a (mapped V44 FY 2027 ICD-10-CM codes and deleted Version (V43) FY 2026 ICD-10-CM codes) and 6P.1b (mapped V44 FY 2027 ICD-10-PCS codes and deleted V43 FY 2026 ICD-10-PCS codes). These mapping files support hospitals’ efforts to use the test GROUPER alongside their own claims data to develop claims-based scenarios to evaluate the impact of the proposed changes included in the FY 2027 inpatient and LTCH PPS proposed rule.
As previously expressed, the absence of a batch test GROUPER significantly limits hospitals’ ability to efficiently evaluate the impact of proposed MS-DRG changes. While the availability of updated test software is appreciated, requiring users to enter test cases individually is time-intensive and inherently restricts hospitals’ ability to conduct comprehensive testing across larger, more representative datasets.
In addition to the broader operational limitations described above, several recurring technical issues noted in this proposed rule further underscore the need for batch GROUPER functionality and enhanced transparency to support meaningful evaluation of the proposed changes.
These technical issues include the following:
- Proposed revisions involving the elimination of cluster logic materially alter MS-DRG assignment pathways and limit stakeholders’ ability to accurately model impacts using existing tools.
- Absent recalibration through a batch GROUPER that reflects the proposed logic changes, stakeholders’ ability to conduct reliable analysis is materially limited. This limitation is evident across MDCs in this proposed rule.
- Several proposed GROUPER changes rely on procedure codes that were not included in the FY 2025 claims data used for CMS’s analysis, as these codes became effective in FY 2026. As a result, CMS relied on mapping methodologies to approximate these procedures. However, procedure code mapping inherently introduces limitations, as it requires the use of broader, less specific legacy codes, thereby reducing the precision and reliability of impact estimates. This issue is particularly relevant within Major Diagnostic Categories (MDCs) 05, 08 and 10.
- The absence of clear and consistent “from/to” MS-DRG mappings limits stakeholders’ ability to validate and replicate CMS’ analyses. This limitation is further compounded by observed discrepancies between narrative descriptions of expected MS-DRG shifts and the corresponding data presented in the After Outliers Removed (AOR) file included with the proposed rule materials, which in some instances reflect conflicting directional impacts. This issue is also observed within MDCs 05, 08, and 10.
We appreciate CMS’ acknowledgment and stated future consideration of providing a batch test GROUPER, as noted in its response to comments in the FY 2026 inpatient and LTCH PPS final rule. Given this prior recognition and the technical issues outlined above, we urge CMS to prioritize and provide a batch GROUPER option in conjunction with future rulemaking. Doing so would materially reduce administrative burden, enhance the quality and depth of stakeholder feedback, and support more informed and effective policy development.
FY 2027 MS-DRG Updates
For the FY 2027 IPPS proposed rule, we acknowledge that CMS’s MS-DRG analysis is based on ICD-10 claims data from the September 2025 update of the FY 2025 MedPAR file, which includes hospital bills received from October 1, 2024, through September 30, 2025.
We recognize the level of detail and the significant time and effort CMS dedicates to developing the analysis and supporting materials included in the inpatient and LTCH PPS proposed and final rules related to MS-DRG classification. However, consistent with concerns raised in our comments on the FY 2026 MS-DRG classification proposals, we again note challenges related to transparency, specifically with respect to MS-DRG volume shifts when comparing GROUPER V43 to V44 in the AOR file accompanying this proposed rule.
MDC 05 (Disease and Disorders of the Circulatory System) WiSE®Cardiac Resynchronization Therapy (CRT System)
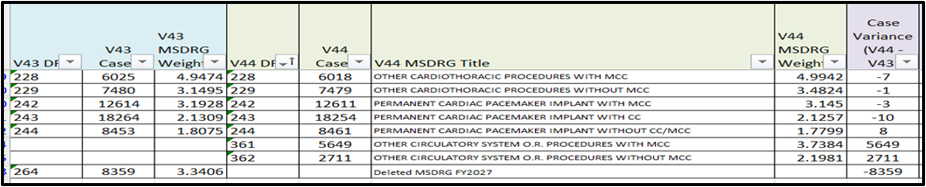
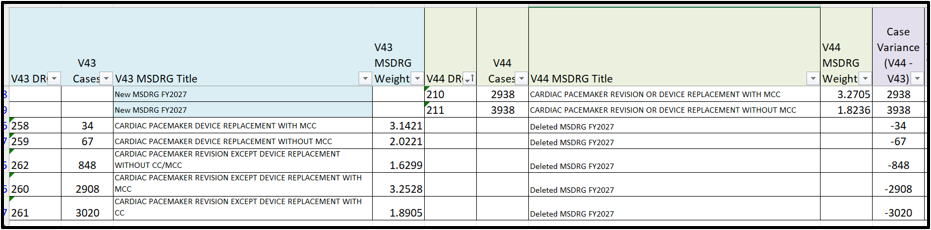
We appreciate CMS’ efforts to modernize MS-DRG classifications within MDC 05. Including the proposed deletion of cardiac pacemaker replacement and revision MS-DRGs (258-262) to consolidate pacemaker replacement and revisions into two new MS-DRGs (210 and 211), as well as the deletion of MS-DRG 264 and the creation of two new MS-DRGs with a two-level severity hierarchy (361 and 362) for other circulatory system O.R. procedures. We also recognize CMS’ intent to refine classification for emerging technologies, including the WiSE® CRT system, through the removal of cluster logic and reassignment of newly established ICD-10-PCS procedure codes.
While we support CMS’ goal of improving MS-DRG clarity and alignment with evolving procedural approaches, we have identified potential inconsistencies between the proposed MS-DRG logic, the ICD-10-PCS procedure code assignments, and the draft V44 GROUPER outcomes. Specifically, CMS proposes that ICD-10-PCS procedure codes associated with the WiSE® CRT system, X2HN37B, would be assigned to MS-DRGs 228 and 229, and XHH80HB would be reassigned to the proposed new MS-DRGs 210 and 211 as standalone procedures, respectively, with the removal of cluster logic.
However, using draft test GROUPER V44 indicates that cases involving pacemaker revision with replacement scenarios (e.g., replacement of generator and leads due to device malfunction or end-of-life) are not consistently grouped to MS-DRGs 210 and 211 as expected. Instead, these cases are assigned to MS-DRGs 242-244 (pacemaker insertion), which appear inconsistent with both the clinical scenario and the intended MS-DRG definitions.
This outcome appears to be driven in part by surgical hierarchy logic, whereby insertion procedures supersede revision with replacement procedures within the grouping algorithm. However, in clinically typical scenarios, pacemaker replacement requires both removal and insertion procedures (e.g., removal of malfunctioning leads and generator with insertion of new components). In these instances, reliance on surgical hierarchy may not appropriately reflect the clinical intent of the procedure (replacement versus initial insertion), resulting in MS-DRG assignments that do not appear to be the intent.
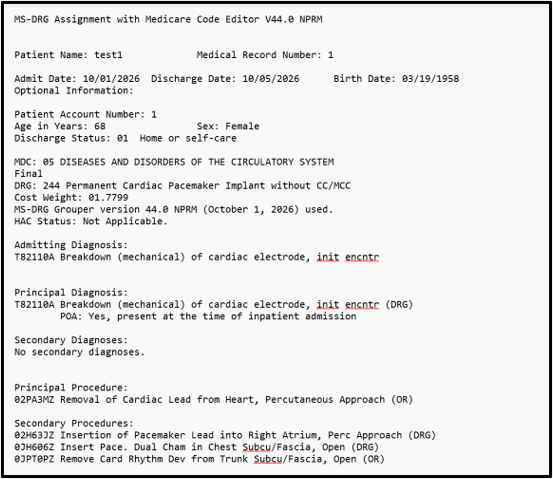
We also identified challenges in replicating CMS’s analysis based on the information provided. Although Table 6P.2a lists the ICD-10-PCS codes proposed for assignment to MS-DRGs 210 and 211, the relationship between those codes and actual V44 GROUPER results cannot be fully validated without additional detail on the logic interactions, including surgical hierarchy rules and the effects of removing cluster requirements. The screenshot below illustrates a pacemaker revision case that groups to pacemaker insertion, even though the procedure codes appear in Table 6P.2a for assignment to MS-DRGs 210 or 211.
Additionally, analysis of the AOR file for MDC 05 demonstrates substantial MS-DRG shifts under the proposed policy, including movements that appear attributable both to severity-level changes (Complication (CC) or Comorbidity/Major Complication (MCC) or Comorbidity CC/MCC refinements) and to structural changes such as the removal of cluster logic. The magnitude and distribution of these shifts make it difficult for hospitals to reliably model financial and operational impacts using standard tools and the case-by-case test GROUPER. (Reference the following excerpt from the AOR file).
CMS indicated in its discussion that cases involving WiSE® CRT procedures would shift into MS-DRGs 228 and 229. However, our review comparing V43 and draft V44 from the AOR file suggests a decline in case volumes within MS-DRGs 228 and 229, as well as in certain pacemaker-related MS-DRGs such as 242 and 243, which appears inconsistent with CMS’ intended expectations. (Reference AOR file excerpts to follow).
These observations raise questions regarding:
- The interaction between reassigned procedure codes and broader MS-DRG logic.
- The role of hierarchy in overriding proposed classification intent.
- Whether additional codes or combinations are driving cases into alternative MS-DRGs not identified in CMS’ narrative.
Absent additional technical detail, it is difficult to reconcile CMS’ projected directional impacts with observed GROUPER and AOR file results.
To ensure clinical coherence, analytic validity and stakeholder confidence in these proposed changes, we respectfully request that CMS:
- Provide detailed technical specifications regarding how ICD-10-PCS procedure codes associated with WiSE® CRT and pacemaker revision/replacement interact with the surgical hierarchy, particularly in cases involving both removal and insertion procedures.
- Assess whether the current surgical hierarchy accurately reflects the clinical intent of device replacement cases, and refine it as needed to avoid classifying replacements as initial insertions.
- Provide additional analytic resources, including:
- A “from/to” MS-DRG crosswalk reflecting proposed logic.
- More detailed AOR file identifying drivers of MS-DRG shifts.
MDC 08 (Diseases and Disorders of the Musculoskeletal System and Connective Tissue) Spinal Fusion and Pelvic Fixation Procedures
We appreciate CMS’ ongoing efforts to refine the MS-DRG classification system to ensure that inpatient cases are grouped in clinically coherent categories that appropriately reflect resource use. However, we wish to highlight a key analytic concern specific to MS‑DRG 426 when evaluating trends across FY 2025 and FY 2026.
In the FY 2025 inpatient PPS final rule, CMS finalized a major restructuring of spinal fusion MS‑DRGs, including the creation of MS‑DRGs 426-428 to describe multi-level non‑cervical combined anterior/posterior spinal fusion cases, along with other new fusion groupings. This redesign effectively established a new cohort definition beginning in FY 2025, rather than a continuation of an existing, stable classification population.
For FY 2026, CMS implemented annual updates to the MS‑DRG GROUPER and Medicare Code Editor (MCE), including the FY 2026 GROUPER and associated classification updates for discharges on or after Oct. 1, 2025. Even when an MS‑DRG title remains unchanged, GROUPER version changes can affect case assignment through updated code logic, edits and classification pathways.
Because FY 2025 established a new MS‑DRG cohort and FY 2026 proceeded under a new GROUPER version, observed shifts in MS‑DRG 426 relative weight and case volume across these two years may reflect classification dynamics rather than true changes in patient acuity or resource use. These dynamics include:
- Stabilization effects following the FY 2025 restructure.
- Evolving coding and documentation patterns under the new fusion constructs.
- GROUPER version changes that affect case routing and logic application.
Accordingly, hospitals attempting to assess payment adequacy, budget neutrality or operational impacts for MS‑DRG 426 across FY 2025 and FY 2026 may reach misleading conclusions if these years are treated as directly comparable.
These considerations are particularly important in the context of CMS’ proposed FY 2027 MS‑DRG weight for MS‑DRG 426, which reflects a notable decrease from prior years. Given the structural and methodological changes described above, we are concerned that this proposed reduction may not fully reflect a stable or mature representation of the underlying case mix and resource use associated with this MS‑DRG.
To support transparent, reproducible analysis by hospitals and stakeholders, we respectfully request that CMS:
- Acknowledge the non-comparability of spinal fusion MS-DRGs across FY 2025, FY 2026 and FY 2027 through a major spinal fusion restructure.
- Provide explicit documentation of any FY 2026 refinements that affect case assignment to MS‑DRG 426, including logic sequencing or edit-driven pathways that could shift cases among related spinal fusion MS‑DRGs.
- Publish supplemental, stakeholder-usable crosswalks and testing support to enable hospitals to evaluate impacts using their own claims under the applicable GROUPER logic (e.g., clarifying which code/logic changes materially alter routing into or out of MS‑DRGs).
- Where feasible, provide comparative impact metrics (e.g., “case movement” summaries between related spinal fusion MS‑DRGs) so stakeholders can distinguish between true acuity/resource shifts and classification-driven redistribution.
- Re-evaluate the proposed FY 2027 MS‑DRG weight (9.2898) for MS‑DRG 426 and exercise caution in relying on FY 2025-FY 2026 data trends as a stable basis for recalibration. Specifically, we urge CMS to consider whether the observed downward weight trend proposed for FY 2027 (FY 2025: 10.4754; FY 2026: 11.0212; FY 2027 proposed: 9.2898) reflects transitional classification effects rather than sustained changes in resource utilization, and to consider maintaining or recalibrating the weight accordingly.
MDC 08 (Diseases and Disorders of the Musculoskeletal System and Connective Tissue) Hip or Knee Procedures with Periprosthetic Joint Infection
As background, in the FY 2026 inpatient and LTCH PPS proposed rule, CMS proposed creating MS‑DRGs 403 and 404 to better capture the complexity of periprosthetic joint infection (PJI) cases involving hip and knee procedures. CMS’ initial analysis found that these cases were not adequately represented in existing MS‑DRGs and supported a two-level severity split.
However, during the FY 2026 rulemaking cycle, stakeholders identified concerns related to inconsistencies in the GROUPER logic. Specifically, commenters noted overlapping procedure code logic between the proposed PJI MS‑DRGs and existing MDC 08 MS‑DRGs for revision hip and knee procedures. CMS subsequently confirmed that certain ICD‑10‑PCS procedure code cluster restrictions were limiting case assignment and interfering with intended clinical groupings.
After removing these restrictions and conducting additional analysis, CMS observed significant redistribution of cases across multiple MS‑DRGs, which reduced case volumes and affected the integrity of existing severity splits. CMS determined that addressing these issues would require more extensive restructuring of MDC 08 and therefore did not finalize the proposal for FY 2026 due, in part, to the lack of updated test GROUPER results available for stakeholder evaluation.
For FY 2027, CMS again proposes to establish MS‑DRGs 403 and 404 for PJI cases and indicates that it has addressed prior concerns through technical refinements. We appreciate CMS’ continued efforts to improve the clinical coherence and payment accuracy of MS‑DRG classifications for cases involving hip or knee procedures complicated by PJI. We support CMS’ goal of better aligning MS-DRG assignments with patient complexity, resource use and severity of illness.
At the same time, we have significant concerns regarding both 1) the transparency and replicability of the proposed methodology and 2) the resulting clinical coherence of MS‑DRG groupings following these changes, particularly as they relate to the redistribution of cases across existing MS‑DRG families.
CMS indicates that the proposed reassignment of cases is driven in part by the removal of MDC 08 “cluster restriction” logic within MS‑DRGs 466-468 and 485-487, which alters how procedure code attributes are evaluated and affects assignment through the surgical hierarchy. These same MS-DRGs are proposed for deletion after the removal of the cluster logic, and new MS-DRGs 400, 403, 404 and 449 are proposed.
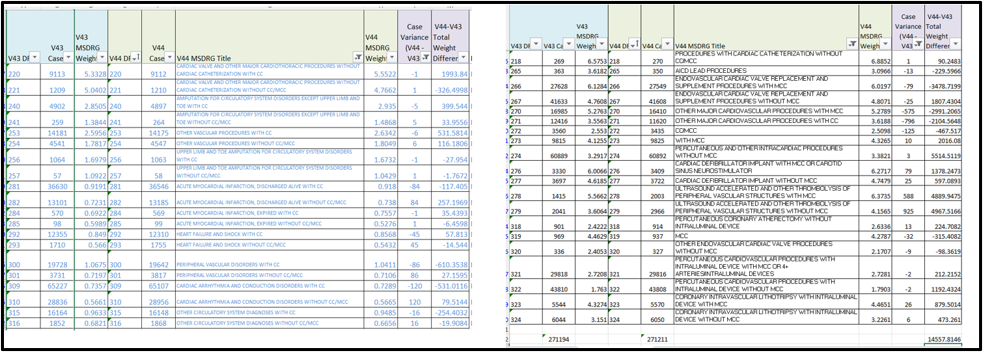
Our review of the AOR file demonstrates that MS-DRGs 466, 467, 468, 485, 486 and 487 for V43 of the GROUPER total 42,703 cases; however, the case total for the new MS-DRGs only totals 16,374. The proposal does not indicate the existing MS-DRGs to which the remaining 26,329 cases will shift.
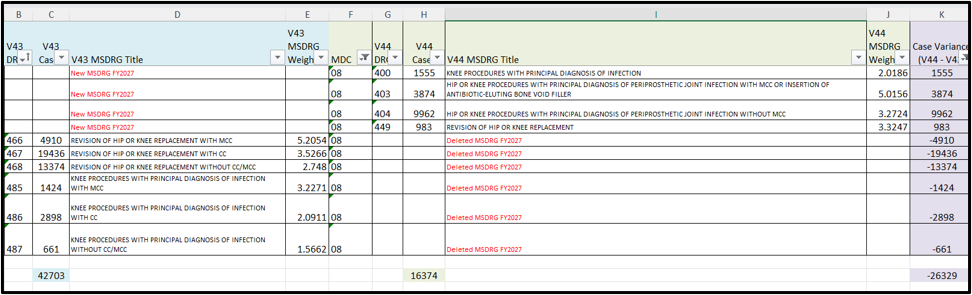
The AOR file also provides some information regarding the shifts and demonstrates shifts within multiple MS-DRGs within MDC 08.
Our review of the AOR file indicates substantial shifts in case volume across MS‑DRG families, including:
- A significant increase in case volume for MS-DRGs 463-465 (Wound Debridement or Skin Graft).
- A substantial decrease in case volume for MS-DRGs 489, 488 and 481 (knee procedures without a principal diagnosis of infection and hip/femur procedures, except major joint).
However, while CMS describes the mechanism at a high level, the proposal context does not provide sufficient detail for stakeholders to fully understand, replicate or validate the resulting case movements across MS‑DRGs.
While these aggregate changes are observable, stakeholders cannot independently determine:
- Which specific cases are shifting?
- Which procedure codes and code clusters are driving the reassignment?
- How do surgical hierarchy and cluster attribute changes interact to produce the observed outcome?
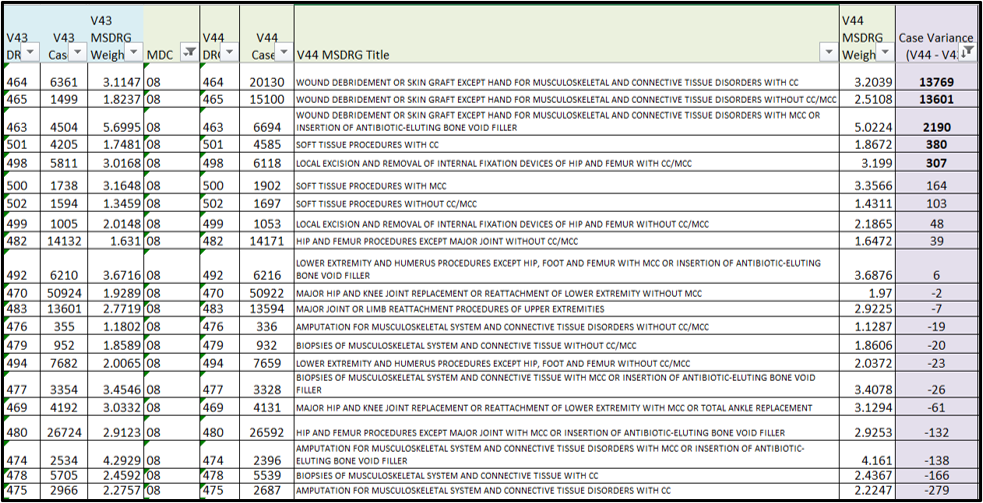
In addition to transparency issues, we question the clinical coherence of the resulting MS-DRG assignments, particularly the significant redistribution of cases into MS-DRGs 463-465 (Wound Debridement or Skin Graft Except Hand). The substantial increase in volume within these existing debridement MS-DRGs will negatively affect data comparability over time.
Analysis of the AOR file comparing debridement MS-DRGs between V43 and V44 reflects an increase of 29,560 cases under the proposed GROUPER. It is unclear why new MS-DRGs were not considered to account for this shift. Under the proposal, these MS-DRGs would absorb a materially different case mix, including hip and knee procedures, which were not represented in prior versions of these DRGs. (Reference the AOR file excerpt to follow).
Given that these changes rely on upstream GROUPER mechanics, specifically the interaction between procedure code clusters, MDC restrictions, and hierarchy precedence, this lack of transparency significantly limits the ability of hospitals to conduct reliable, apples‑to‑apples impact analyses, evaluate payment implications or validate CMS’ conclusions.
To support meaningful stakeholder evaluation, we respectfully request that CMS provide:
- Consider whether new or refined MS-DRGs are warranted to distinguish differences with debridement MS-DRGs 463, 464 and 465 that reflect the new MS-DRG shifts.
- Consider whether the proposed redistribution into MS‑DRGs 463-465 appropriately reflects clinical similarity and resource use, or whether further refinement of logic lists or hierarchy is needed.
- Provide a comprehensive “from/to” crosswalk showing case counts moving from each MS‑DRG under the current GROUPER V43 to each MS‑DRG under the proposed GROUPER V44, with specific alignment to the populations defined in Table 6P.3b.
Lastly, for MDC 08, we note that CMS acknowledges the proposed implementation of a new ICD‑10‑PCS procedure code (XW0V0BC) effective October 1, 2026, to describe the administration of CERAMENT® V, an antibiotic‑eluting bone void filler containing vancomycin, in contrast to the existing code XW0V0P7, which describes CERAMENT® G (gentamicin).
In the proposed rule, CMS recognizes that cases involving the use of antibiotic‑eluting bone void fillers are associated with higher resource utilization. Accordingly, we request that CMS apply a consistent policy approach, designating this new code as non-O.R., impacting MS-DRG so that it groups with the MS-DRGs that recognize the antibiotic-eluting bone void filler (e.g., 463, 474, 477, 480, 492, 616, 628).
Read the full letter below.
__________
1 AHA. (March 2026). The Cost of Caring: Challenges Facing America’s Hospitals as They Care for Patients in 2026 (https://www.aha.org/costsofcaring).
2 Id.
3 Id.
4 Id.
5 https://premierinc.com/newsroom/policy/claims-adjudication-costs-providers-257-billion-18-billion-is-potentially-unnecessary-expense
6 DHHS OIG. (2023). High Rates of Prior Authorization Denials by Some Plans and Limited State Oversight Raise Concerns About Access to Care in Medicaid Managed Care. https://oig.hhs.gov/oei/reports/OEI-09-19-00350.pdf
7 MedPAC (2021). MedPAC Report to Congress. https://www.medpac.gov/wp-content/uploads/import_data/scrape_files/docs/default-source/reports/mar21_medpac_report_to_the_congress_sec.pdf#page=401
8 Ensemble Health Partners. (2023). The Real Cost of Medicare Advantage Plan Success. https://www.ensemblehp.com/blog/the-real-cost-of-medicare-advantage-plan-success/
9 MedPAC. (2026). https://www.medpac.gov/wp-content/uploads/2026/03/Mar26_Ch3_MedPAC_Report_To_Congress_SEC.pdf
10 Challenges Facing America’s Hospitals as They Care for Patients in 2026 (https://www.aha.org/costsofcaring).
11 85 Fed. Reg. 58797 (Sept. 18, 2020).
12 91 Fed. Reg. 19484 (April 14, 2026).
13 Page 19. https://www.cms.gov/research-statistics-data-and-systems/statistics-trends-and-reports/reportstrustfunds/downloads/technicalpanelreport2010-2011.pdf
14 90 Fed. Reg. 18257 (April 30, 2025).
15 https://www.nytimes.com/2024/03/24/opinion/prior-authorization-medical-care.html; https://www.nbcnews.com/health/rejecting-claims-medicare-advantage-rural-hospitals-rcna121012; https://www.npr.org/sections/health-shots/2023/10/17/1205941901/medicare-advantage-rural-hospitals; https://www.beckershospitalreview.com/finance/nearly-half-of-health-systems-are-considering-dropping-ma-plans.html
16 “NHE Projections – Tables.” https://www.cms.gov/data-research/statistics-trends-and-reports/national-health-expenditure-data/projected
17 https://www.kff.org/affordable-care-act/what-we-know-so-far-about-2026-aca-marketplace-enrollment-premiums-and-deductibles/
18 https://www.cbo.gov/system/files/2025-06/Arrington-Guthrie-Letter-Medicaid.pdf
19 https://www.urban.org/research/publication/obbbas-six-month-redetermination-could-reduce-medicaid-expansion-enrollment-20
20 https://www.cbo.gov/system/files/2025-08/61367-Uninsured-Data.xlsx
21 https://www.aha.org/lettercomment/2021-06-28-aha-comments-inpatient-pps-proposed-rule-fy-2022
22 https://www.aha.org/lettercomment/2022-06-17-comments-cms-its-fy-2023-proposed-inpatient-prospective-payment-system
23 https://www.aha.org/lettercomment/2023-05-01-aha-letter-cms-medicare-disproportionate-share-hospital-payments-section-1115
Key Resources
Related Resources
Webinar Recordings