

Unwise DSH Cuts Combined with Rise in Uncompensated Care Due to Medicaid Redeterminations Coverage Losses Further Threaten Hospitals’ Financial Stability

More than 90 million people had access to health care through Medicaid’s pandemic-related continuous coverage provisions. That coverage ended March 31, 2023, and states have since resumed normal Medicaid eligibility redetermination processes. The Medicaid program now faces the most significant coverage challenge in more than a decade. While the complete impact is still unfolding, these redeterminations have already resulted in millions of people losing their Medicaid eligibility.
Although a portion of those disenrolled from Medicaid may find coverage alternatives, it is expected that a substantial number will unfortunately face a complete loss of coverage. Emerging data suggests that Medicaid disenrollment is already translating to coverage losses and gaps, leaving patients unable to pay for their care. In addition, those who are enrolled in other coverage, such as a plan offered by their employer or through the Health Insurance Marketplaces, may face increased – and sometimes unaffordable – cost-sharing.
Consequently, over the past few months, hospitals have started to see a substantial increase in uncompensated care. In the wake of the onset of redeterminations, the median rate of uncompensated care for hospitals nationally increased by a third from 6.4% in the first quarter of 2023 to 8.7% in July (see Figure 1), according to data from Syntellis Performance Solutions. For hospitals in states that have not yet expanded Medicaid, and where rates of uncompensated care were already elevated relative to the field, these existing trends have been amplified.
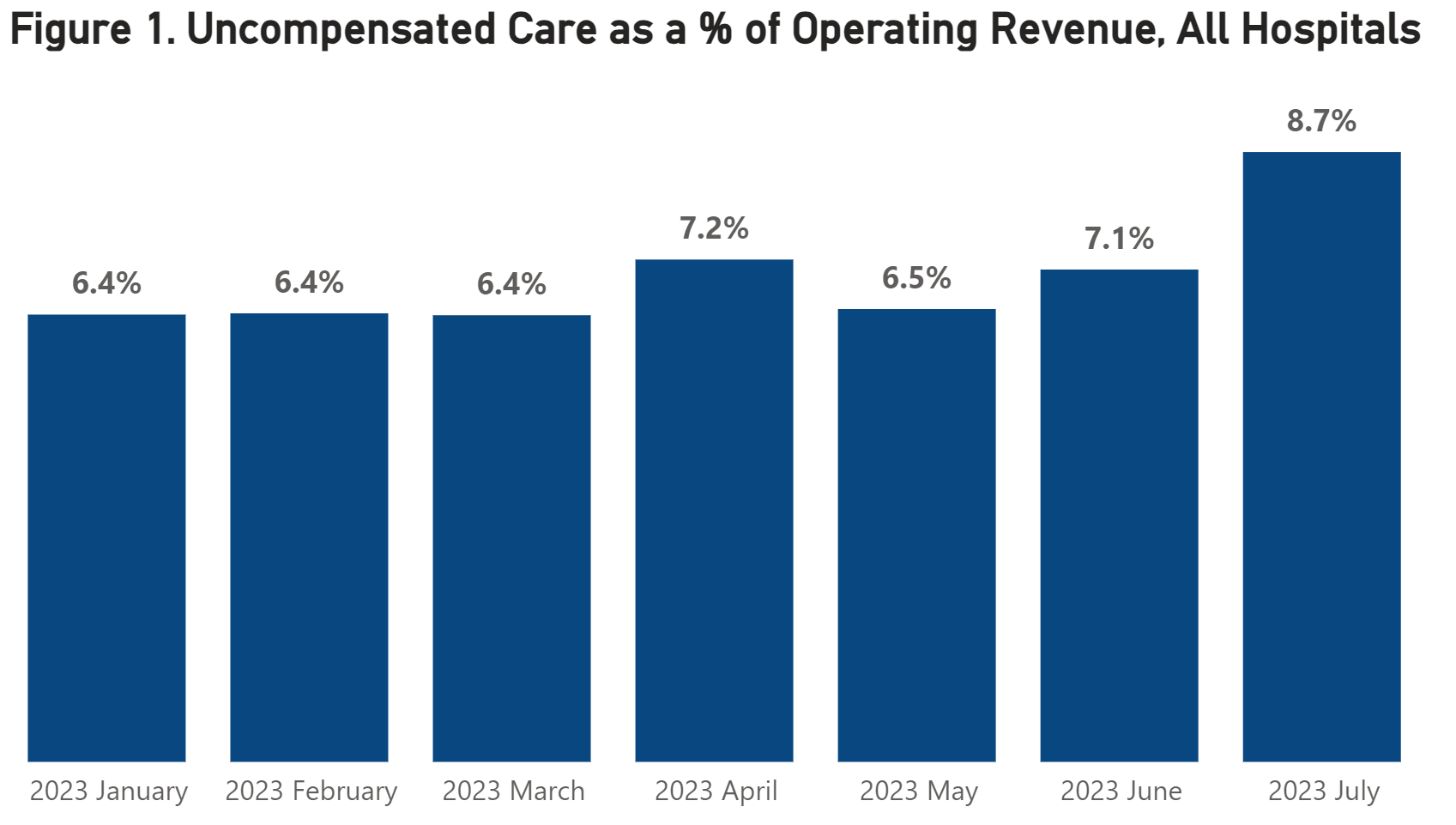
Source: Syntellis Performance Solutions
In addition to increased uncompensated care, these coverage losses also will likely lead to some patients who cannot pay for care to delay seeking necessary medical attention. The deferral of care invariably results in worsening patient health, which frequently requires more complex treatment. If patient health worsens, hospitals must allocate more resources to treat them, which increases in the cost of caring for them.
Although it will take time for the impacts of the Medicaid redetermination process on the health care system to be fully realized, these early and alarming trends in uncompensated care have put further financial strain on hospitals as they struggle to combat rising expenses.
In 2022, over half of hospitals ended the year with negative operating margins. For hospitals serving larger numbers of underserved and historically marginalized populations, these trends in uncompensated care are even more troubling. Coverage losses will have a disproportionate effect on these hospitals.
In recent letters to states, the Centers for Medicare & Medicaid Services asked for assurance that their Medicaid eligibility redeterminations processes are not resulting in eligible individuals being improperly disenrolled. We share CMS’ concerns about improper disenrollment, and we support the agency’s efforts to provide states with the tools and technical assistance to guard against loss of eligibility.
Despite the foreseeable impact the loss of Medicaid coverage would have on hospitals serving a disproportionate share of low-income patients, CMS recently finalized nearly $1 billion in Medicare funding cuts to disproportionate share hospitals (DSH). These cuts from CMS are predicated on the assumption that the uninsured rate will decline in fiscal year 2024 despite the ongoing redeterminations and recent Congressional Budget Office projections to the contrary. These cuts are happening at a critical time for hospitals and the patients they serve who are struggling to afford care, and we urge CMS to maintain the uninsured rate at FY 2023 levels for FY 2024 in its Medicare DSH calculations.
It is imperative that patients continue to have access to care regardless of their ability to pay. These payment cuts threaten the financial stability of hospitals across the nation, forcing many to consider shutting down vital service lines or risk closing their doors altogether. At a minimum, the Medicaid eligibility redetermination process should be allowed to finish before these Medicare cuts are enacted.
Ari Levin is AHA’s director of coverage and state issues forum. John Allison is AHA’s associate director of health analytics policy.