

Advancing Health Podcast
AHA Comments on DHS Proposed H-1B Visa Weighted Selection Process
October 24, 2025
Joseph B. Edlow
Director, U.S. Citizenship and Immigration Services
U.S. Department of Homeland Security
5900 Capital Gateway Drive
Camp Springs, MD 20746
Submitted Electronically
RE: Weighted Selection Process for Registrants and Petitioners Seeking to File Cap-Subject H-1B Petitions (USCIS-2025-0040), Sept. 24, 2025
Dear Director Edlow:
On behalf of our nearly 5,000 member hospitals, health systems and other health care organizations, our clinician partners — including more than 270,000 affiliated physicians, 2 million nurses and other caregivers — and the 43,000 health care leaders who belong to our professional membership groups, the American Hospital Association (AHA) appreciates the opportunity to comment on the Department of Homeland Security’s (DHS) proposed weighted selection process for registrants and petitioners seeking to file cap-subject H-1B petitions.
DHS’s proposed regulation would replace the current random lottery selection process for H-1B petitions with a weighted selection process based on wage levels. DHS would assign greater weight in the selection process to petitions at higher wage levels, thereby increasing the probability that those petitions are ultimately awarded visas under the H-1B visa program’s statutory caps. Specifically, petitions at the Department of Labor’s Occupational Employment and Wage Statistics Survey (OEWS) wage level IV for a given occupation and location would be entered into the selection pool four times, level III three times, level II two times and level I one time.
The AHA appreciates that DHS’s goal in proposing a weighted selection process is to ensure the H-1B visa program fills labor shortages in positions requiring highly skilled or highly educated workers. However, the revised policy could inadvertently hinder the ability of hospitals to use the H-1B program to fill critical shortages of highly skilled health care workers and ultimately hamper access to care. The impacts could be especially significant for hospitals serving rural and other underserved communities that are already experiencing significant staffing shortages. The AHA recommends thatDHS automatically weigh occupations under medicine and health categories at the equivalent of wage level IV. In other words, we recommend that DHS enter unique beneficiaries who fall under the health care practitioner, health care technical and health care support standard occupational codes (SOCs) into the selection pool four times, regardless of wage level.
Communities across America depend on a highly qualified and trained health care workforce to ensure access to quality care. Hospitals and health systems require staffing 24 hours per day, seven days per week, to remain open. However, hospitals and health systems continue to face critical shortages of physicians, nurses, clinical laboratory experts and other highly skilled and educated health care professionals. For example:
- A recent report from the Health Resources & Services Administration showed that the U.S. is projected to have a shortage of 187,130 full-time equivalent physicians by 2037, with rural or non-metro areas experiencing greater shortages than other parts of the country.1
- The National Center for Health Workforce Analysis projects a 6% shortage of registered nurses nationwide, with a 13% shortage in non-metro areas by 2037.2
- The most recent comprehensive survey from the American Society of Clinical Pathology highlights average vacancy rates of between 7% and 18% for laboratory personnel.3
These shortages have been exacerbated by increased burnout and early retirements, decreasing the supply of clinicians and staff, while demand continues to rise with an aging population. Hospitals have responded to these challenges with robust efforts to bolster recruitment and retention and have invested in increasingly higher wages despite the substantial financial headwinds they continue to face.4
While hospitals and health systems are committed to investing in training the next generation of health care workers, the H-1B visa program is a critical short-term approach used by hospitals to recruit highly skilled health care professionals and maintain access to care in their communities. Of the nearly 400,000 H-1B petitions approved in fiscal year 2024, 16,937 of those, or 4.2% of the total filed petitions, were for medicine and health occupations (including physicians, therapists, pharmacists and other allied health professionals). Many of these petitions fall under the H-1B program’s statutory caps and would be affected by the proposed rule. Foreign-trained medical professionals do not displace American workers. Instead, they play a critical role in improving the health of the communities our hospitals serve. They are highly qualified, required to meet our nation’s standards for education, English fluency and state licensure.
Salaries and wage levels for health care workers vary significantly among different occupation types and across geographies. The latest congressional report from U.S. Customs and Immigration Services on the characteristics of those receiving H-1B visas shows that occupations in medicine and health had the largest variation in annual compensation between the 25th and 75th percentiles among the occupations included in their analysis.5 Additionally, the report showed that the 2024 annual compensation for health care workers in the 25th and 50th percentiles was $20,000 lower than the annual compensation across all workers in the 25th and 50th percentiles.6
To further gauge the impact of the proposed weighted selection process, AHA reviewed publicly available data from the Department of Labor on OEWS wage levels for H-1B recipients. While these data are incomplete, they suggest that most health care occupations would see significantly reduced chances of getting H-1B visas if DHS’ policy were finalized as proposed.
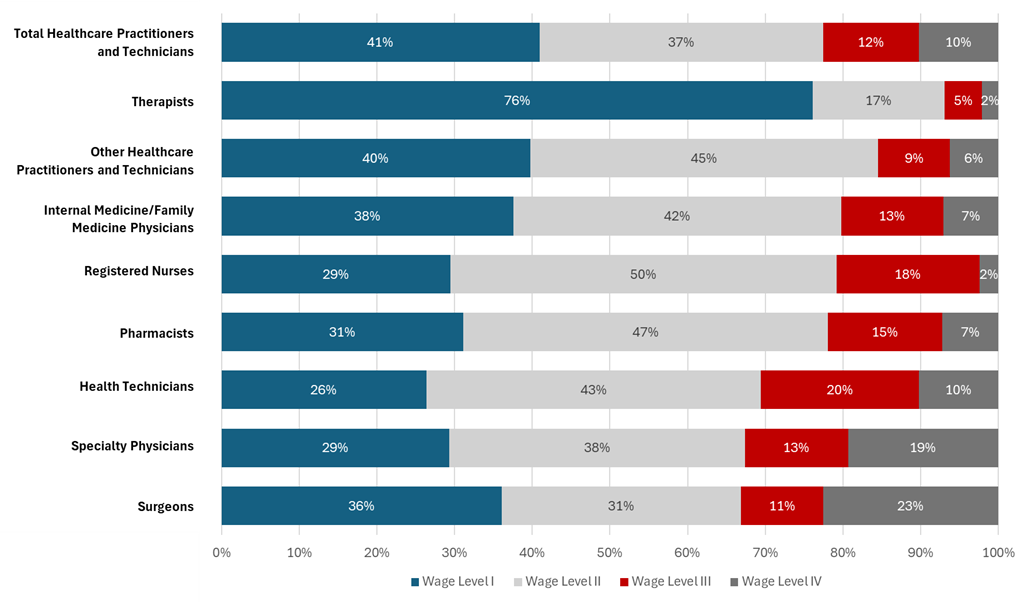
- Indeed, 78% of H-1B health care practitioners and technical occupations were at OEWS wage levels I and II in 2025 (see Figure 1).
- Across all health care practitioner and technical occupational categories, including pharmacists, technicians, physicians and therapists, 67% of H-1B workers were in wage levels I and II.
- Despite representing a small fraction of H-1B petitions, health care workers only represented 2.3% of those in wage level IV, which would receive the highest weight in DHS’ proposed selection process.
These data demonstrate that staffing levels for certain health care occupations could be adversely impacted by the proposed changes to the selection process, since these roles have higher proportions of workers in lower OEWS wage levels and would therefore have a lower likelihood of selection
Figure 1. Percentage of Certified H-1B Visas in Each Wage Level Category for Health Care Practitioners and Technical Occupations in 20257
Hospitals and health systems would also face unique challenges in raising the OEWS wage levels for H-1B recipients. The OEWS levels are based on prevailing wage levels for all workers, not just those receiving H-1B visas, and is determined independent of any foreign training or experience. As a result, H-1B recipients in health care are generally paid at the level corresponding to their U.S. experience — which is often none — despite their substantial training and expertise abroad. In addition, some states may require international clinicians to work a certain number of supervised clinical hours or to pass certain exams or certification before taking on full practice authority, which may limit the initial salary for such clinicians.
The weighted selection process, as currently proposed, also could be especially detrimental to rural and underserved areas. Hospitals and health systems serving these areas face substantial financial headwinds, placing constraints on their ability to pay higher wages that could increase the probability of receiving H-1B visas in a weighted selection process. For all the above reasons, the AHA believes that automatically weighing all health care workers at a level IV will provide the best opportunity for these critical staff to be selected to ensure continued access to care.
The AHA thanks DHS for the opportunity to comment on this proposed rule. We stand ready to work with the agency on ways to ensure any changes to H-1B policy support access to care in communities across America. Please contact me if you have questions at ademehin@aha.org.
Sincerely,
/s/
Akinluwa (Akin) A. Demehin
Vice President
Quality and Safety Policy
1 https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/state-of-the-health-workforce-report-2024.pdf
2 https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/state-of-the-health-workforce-report-2024.pdf
3 https://academic.oup.com/ajcp/article/161/3/289/7344701?guestAccessKey=0b6afc62-1497-493a-b4da-787029afb078
4 https://www.aha.org/costsofcaring
5https://www.uscis.gov/sites/default/files/document/reports/ola_signed_h1b_characteristics_congressional_report_FY24.pdf
6 The annual compensation for the 25th percentile of health care workers was $69,000 compared to the annual compensation for the 25th percentile across occupational categories ($90,000). The annual compensation for the 50th percentile of health care workers was $100,000 compared to the annual compensation for the 50th percentile across occupational categories ($120,000).
7 Q3 2025 Department of Labor LCA Programs (H-1B, H-1B1, E-3) Public Disclosure Data. H-1B Visa Class, Certified Case Status, SOC codes in Healthcare Practitioner and Technical Occupations https://www.dol.gov/agencies/eta/foreign-labor/performance. Analysis excludes individuals for which the OEWS wage level is left blank or marked N/A.