Webinar Recordings
April 2025
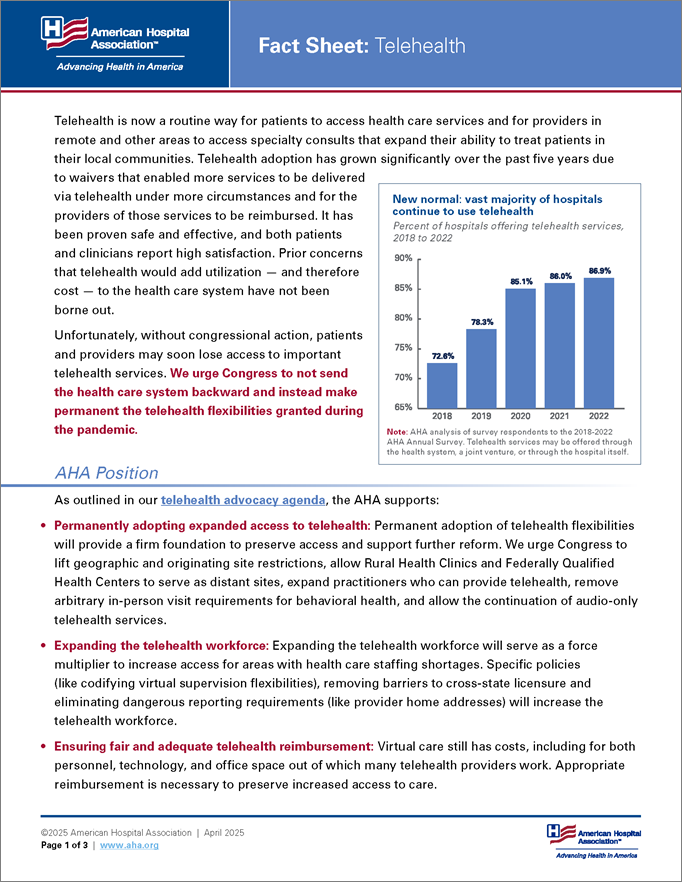
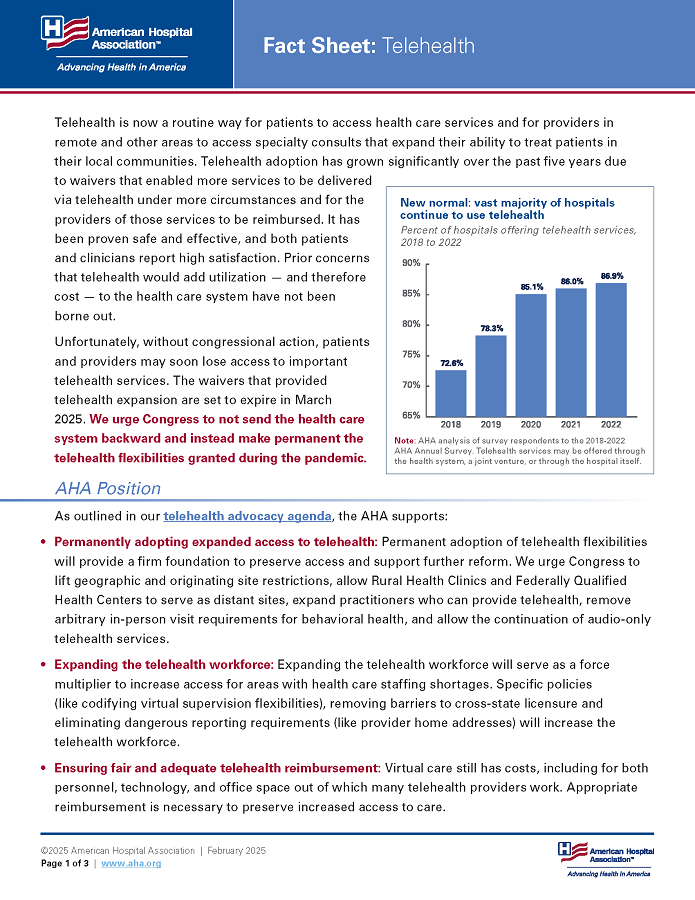
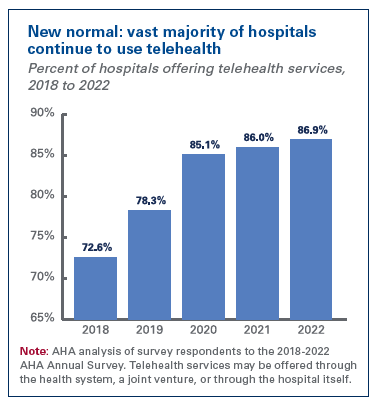 Telehealth is now a routine way for patients to access health care services and for providers in remote and other areas to access specialty consults that expand their ability to treat patients in their local communities. Telehealth adoption has grown significantly over the past five years due to waivers that enabled more services to be delivered via telehealth under more circumstances and for the providers of those services to be reimbursed. It has been proven safe and effective, and both patients and clinicians report high satisfaction. Prior concerns that telehealth would add utilization — and therefore cost — to the health care system have not been borne out.
Telehealth is now a routine way for patients to access health care services and for providers in remote and other areas to access specialty consults that expand their ability to treat patients in their local communities. Telehealth adoption has grown significantly over the past five years due to waivers that enabled more services to be delivered via telehealth under more circumstances and for the providers of those services to be reimbursed. It has been proven safe and effective, and both patients and clinicians report high satisfaction. Prior concerns that telehealth would add utilization — and therefore cost — to the health care system have not been borne out.
Unfortunately, without congressional action, patients and providers may soon lose access to important telehealth services. We urge Congress to not send the health care system backward and instead make permanent the telehealth flexibilities granted during the pandemic.
As outlined in our telehealth advocacy agenda, the AHA supports: