

Guides/Reports
October 2021
Hospitals and health systems work hard every day to make care more cost-effective and efficient for their patients, at the same time that they are caring for the nation’s most complex and resource-intensive patients. This has been especially true during the COVID-19 pandemic as hospitals and health systems have provided essential services and saved lives, while also facing unprecedented financial and operational challenges.
In recent years, health care spending growth has largely been driven by increased use and intensity of services.
In 2019, increased use and intensity of services was the primary driver for health care spending growth.
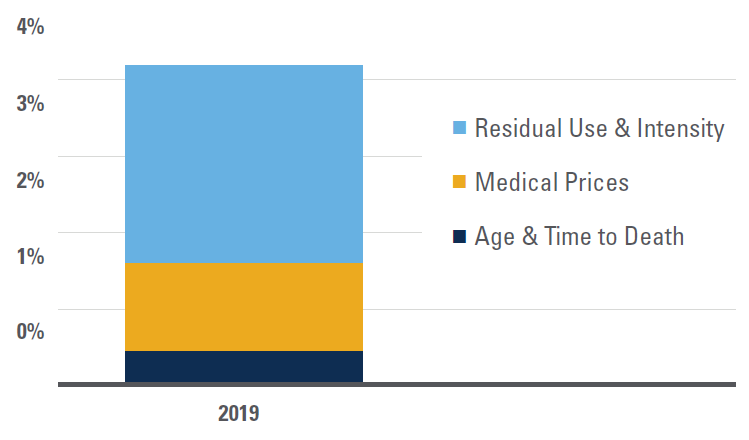
Source: Centers for Medicare and Medicaid Services, Office of the Actuary, National Health Statistics Group. <Note: Medical price growth, which includes economywide and excess medical-specific price growth (or changes in medical-specific prices in excess of economywide inflation), is calculated using the chain-weighted NHE price deflator. “Residual use and intensity” is calculated by removing the effects of population, demographic factors (age and time to death), and price growth from the nominal expenditure level.
Health insurance premiums have generally grown more than double the rate of hospital prices over the last decade.
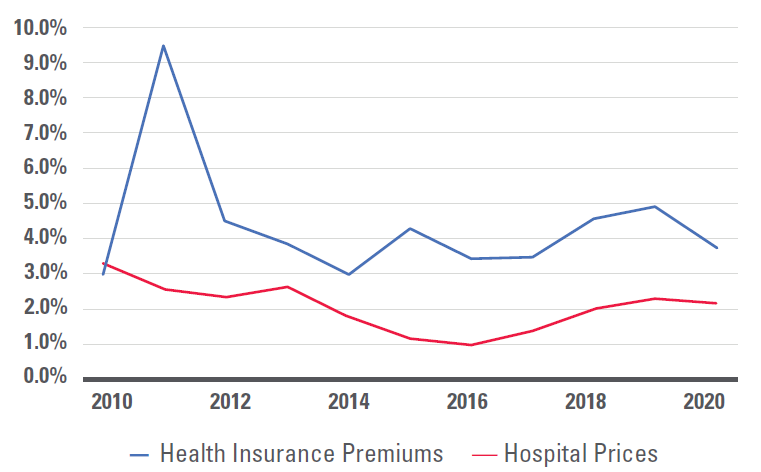
Source: Health insurance premiums represent premiums for a family of four, from KFF Employer Health Benefits Survey, 2018-2020, and Kaiser/HRET Survey of Employer Health Benefits (2007-2017). Hospital prices: Bureau of Labor Statistics, Produce Price Index data, 2007-2020 for Hospitals (series ID 622).
Hospital care requires a range of inputs such as wages, prescription drugs, food, medical devices, utilities and professional insurance. Steep increases in input prices, like rapidly escalating drug prices, can undermine hospitals’ efforts to reduce the cost of care.
Employee wages and benefits constitute the largest percentage of costs for inpatient hospital services.
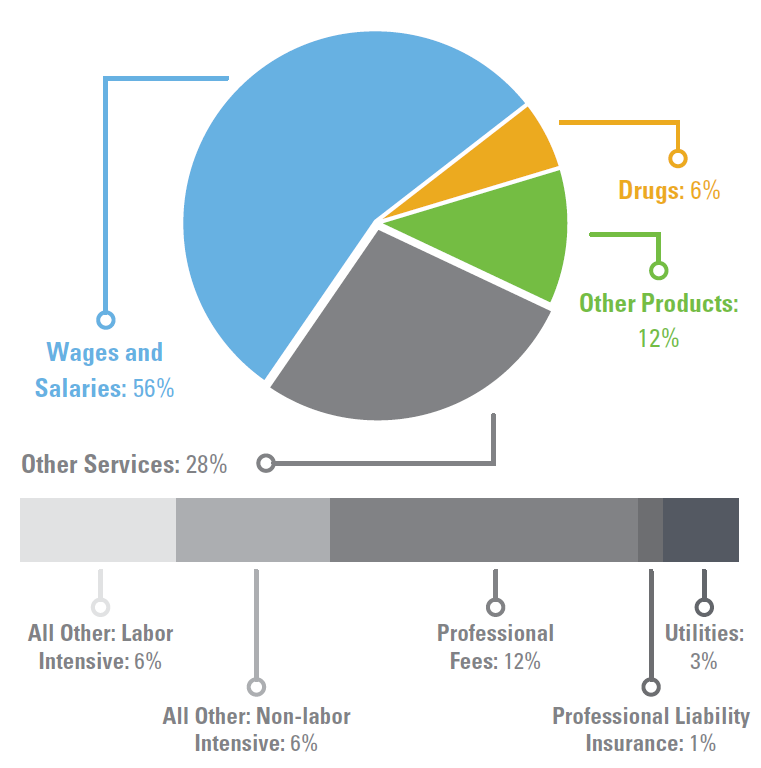
Source: AHA Analysis of Centers for Medicare & Medicaid Services FY18 IPPS Market Basket Data, Using base year 2014 weights. (1) Does not include capital. (2) Includes postage and telephone expenses.
Changes in Expense YTD as Compared with Pre-Pandemic Levels
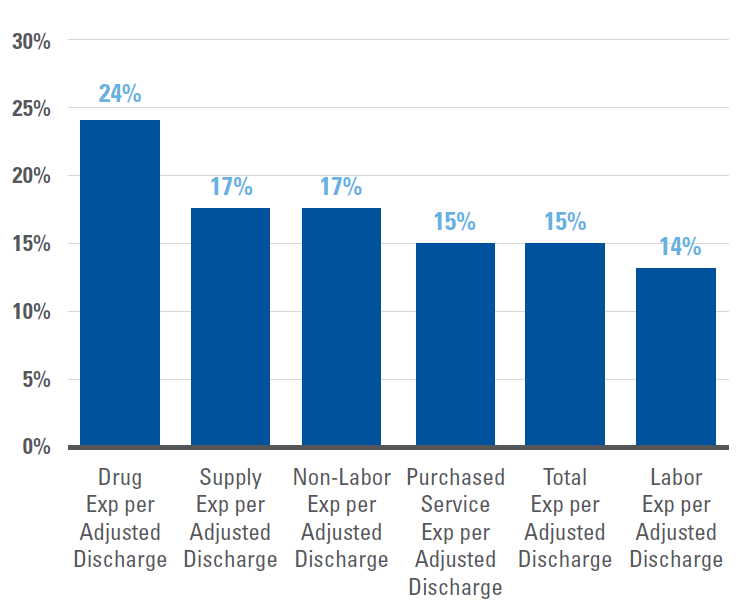
Source: Kaufman Hall's September 2021 Report "Financial Effects of COVID-19: Hospital Outlook for the Remainder of 2021.”
The COVID-19 pandemic heightened a number of these pressures, with significant challenges and economic uncertainty remaining.
To learn more about how hospitals are driving value and affordability, and how the AHA is promoting these principles, visit: https://www.aha.org/issue-brief/2019-09-18-real-affordability-solutions-front-lines-caring.
Real Affordability Solutions from the Front Lines of Caring
Partnerships, Mergers, and Acquisitions Can Provide Benefits to Certain Hospitals and Communities
Financial Effects of COVID-19: Hospital Outlook for the Remainder of 2021
Results from 2018 Tax-Exempt Hospitals’ Schedule H Community Benefit Reports
Perspective: Confronting Commercial Insurers’ Practices that Threaten Patient Care
Lown Institute Report on Hospital Community Benefits Falls Short
Study: Health insurance market becoming more concentrated
Report: American Medical Association Report on Competition in the Health Insurance